Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Erosive hand osteoarthritis (EHOA) is an inflammatory subtype of hand OA that causes subchondral bone erosion and cortical destruction, often resulting in debilitating symptoms. The association between inflammation, dysregulated immunity and cardiovascular event (CVE) risk is well established1. Specifically, several previous studies have found an increased risk of CVE in patients with rheumatoid arthritis (RA)2. Given the common denominator of inflammation in RA and EHOA, we hypothesized that EHOA is associated with increased CVE risk.
Methods: Patients with EHOA were identified from the electronic medical record by ICD code or by utilizing radiograph reports containing the term “erosive osteoarthritis”. Radiographs were reviewed to confirm the characteristic changes of EHOA, namely central erosions and joint space narrowing within the distal and middle interphalangeal joints. Patients with autoimmune arthritis were excluded. Age and gender matched controls were identified in a 1:3 ratio. Study variables included BMI, smoking history, Type II diabetes and statin use. The primary outcome was any cardiovascular disease, while secondary outcomes were myocardial infarction (MI), hypertension (HTN), arterial disease, atherosclerosis, ischemic heart disease or cerebral infarction that were identified using ICD-9 and ICD-10 codes. EHOA and control groups were univariately compared using equal variance two-sample t-tests for continuous variables and Chi-square tests for categorical variables. Differences between cases and controls was estimated using logistic regression modeling adjusted for BMI and smoking history.
Results: We observed a positive association between EHOA and history of 1) any CVE, 2) arterial disease, 3) atherosclerosis, and 4) HTN. The adjusted odds ratio (OR) calculated using multivariate regression analysis was 1.65 (95% CI: (1.15-2.38); p-value 0.007) for overall prevalence of CVE, 1.71 ((95% CI: 1.24-2.37); p-value 0.001) for arterial disease, 2.51 ((95% CI: 1.70-3.69); p-value< 0.001) for atherosclerosis and 1.68 ((95% CI: 1.21-2.34); p-value 0.002) for HTN . The OR was similar without adjusting for covariates.
Conclusion: Our study shows that patients with EHOA have a higher prevalence of any CVE compared with age and gender matched controls with and without adjustment for potential confounders. Within CVEs, it shows higher prevalence of arterial disease, atherosclerosis and HTN. Our findings are in agreement with prior studies performed with RA patients, thus reinforcing the link between inflammation and increased cardiovascular link. Further studies are warranted to explore this association between EHOA and cardiovascular disease.
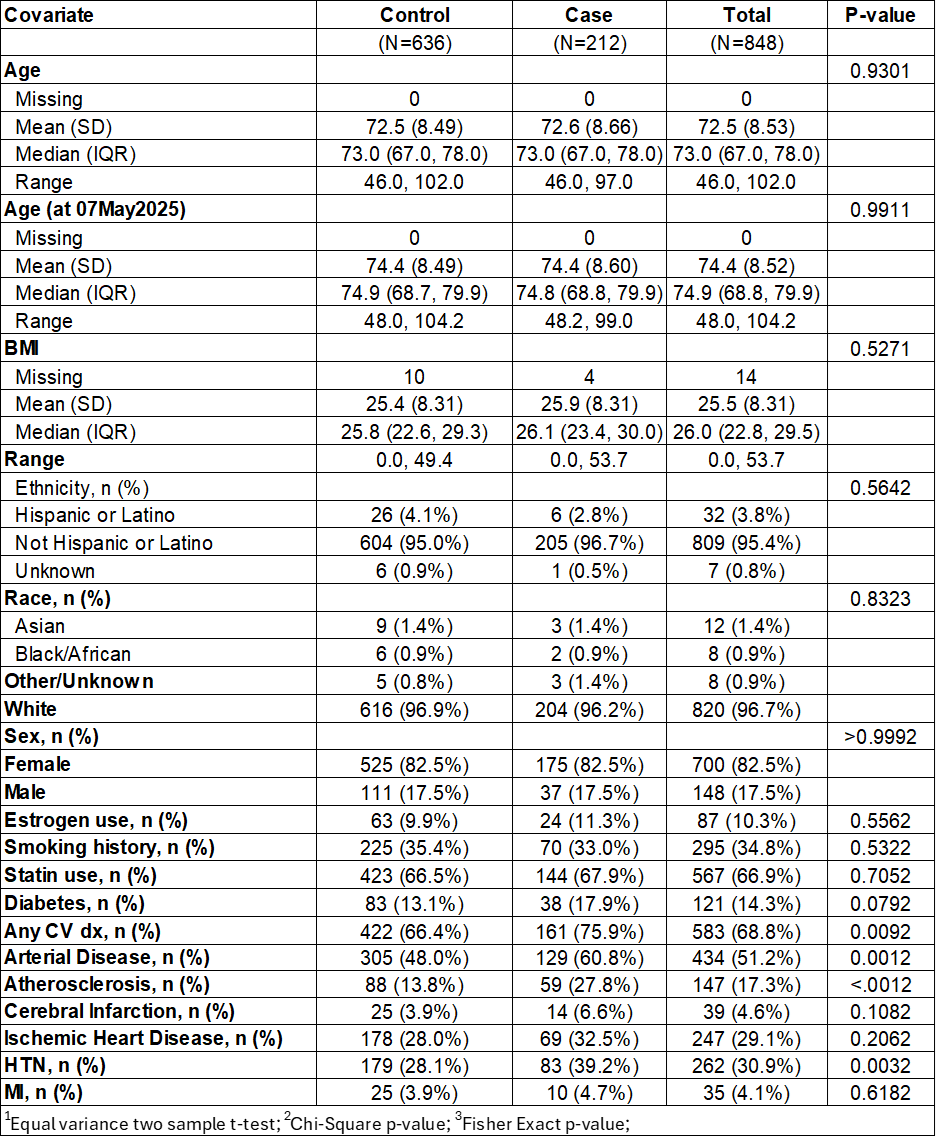 Table 1: Baseline patient characteristics with Descriptive stats and univariate comparison
Table 1: Baseline patient characteristics with Descriptive stats and univariate comparison
(case vs control). Case=EOA patient, Control=non-EOA patient.
.jpg) Table 2: Univariate and multivariable logistic regression modeling (adjusted for BMI, smoking history, statin use, diabetes). Odds ratios and 95% CIs for the case/control status variable listed. Each outcome is modeled separately. Nf848 for each univariate model. Nf834 for each multivariable model (14 pts are missing BMI and excluded from multivariable analysis).
Table 2: Univariate and multivariable logistic regression modeling (adjusted for BMI, smoking history, statin use, diabetes). Odds ratios and 95% CIs for the case/control status variable listed. Each outcome is modeled separately. Nf848 for each univariate model. Nf834 for each multivariable model (14 pts are missing BMI and excluded from multivariable analysis).
To cite this abstract in AMA style:
Mahajan A, Harvey C, Abril A, Sullivan M. Cross-sectional analysis of association between erosive hand osteoarthritis and cardiovascular disease. [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/cross-sectional-analysis-of-association-between-erosive-hand-osteoarthritis-and-cardiovascular-disease/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cross-sectional-analysis-of-association-between-erosive-hand-osteoarthritis-and-cardiovascular-disease/