Session Information
Date: Sunday, November 17, 2024
Title: Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: More than 460 million people worldwide are currently living with prediabetes, a condition that not only predisposes individuals to diabetes (DM) but also to hyperuricemia. Despite the well-established association between prediabetes and hyperuricemia, knowledge about serum urate (SU) trends during the prediabetic phase is limited. Therefore, we assessed the longitudinal changes of SU in individuals with prediabetes.
Methods: We conducted a longitudinal study using electronic health records from Mass General Brigham (2007-2022) to examine SU levels during the prediabetic phase. The study included patients aged ≥18 years with prediabetes, defined by an initial hemoglobin A1c (HbA1c) level between 5.7% and 6.4%, and no prior HbA1c ≥6.5%. The first qualifying HbA1c measurement was the index date. Patients were excluded if they had a history of DM, gout, or used colchicine or urate-lowering therapies within the exclusion window (2005 to the index date). A minimum of 365 days of data before index date and at least one SU test before and after the diagnosis were required.
During follow-up, patients were censored if they developed DM or gout (≥2 ICD codes for gout and/or a gout-specific medication with one diagnostic code). Follow-up continued from the index date until DM onset, gout diagnosis, loss to follow-up, end of the study period, or death. The primary outcome was the trend of SU levels during follow-up, estimated with a multivariable mixed-effects model. We also examined SU variations in subgroups stratified by age, sex, body mass index (BMI), and HbA1c.
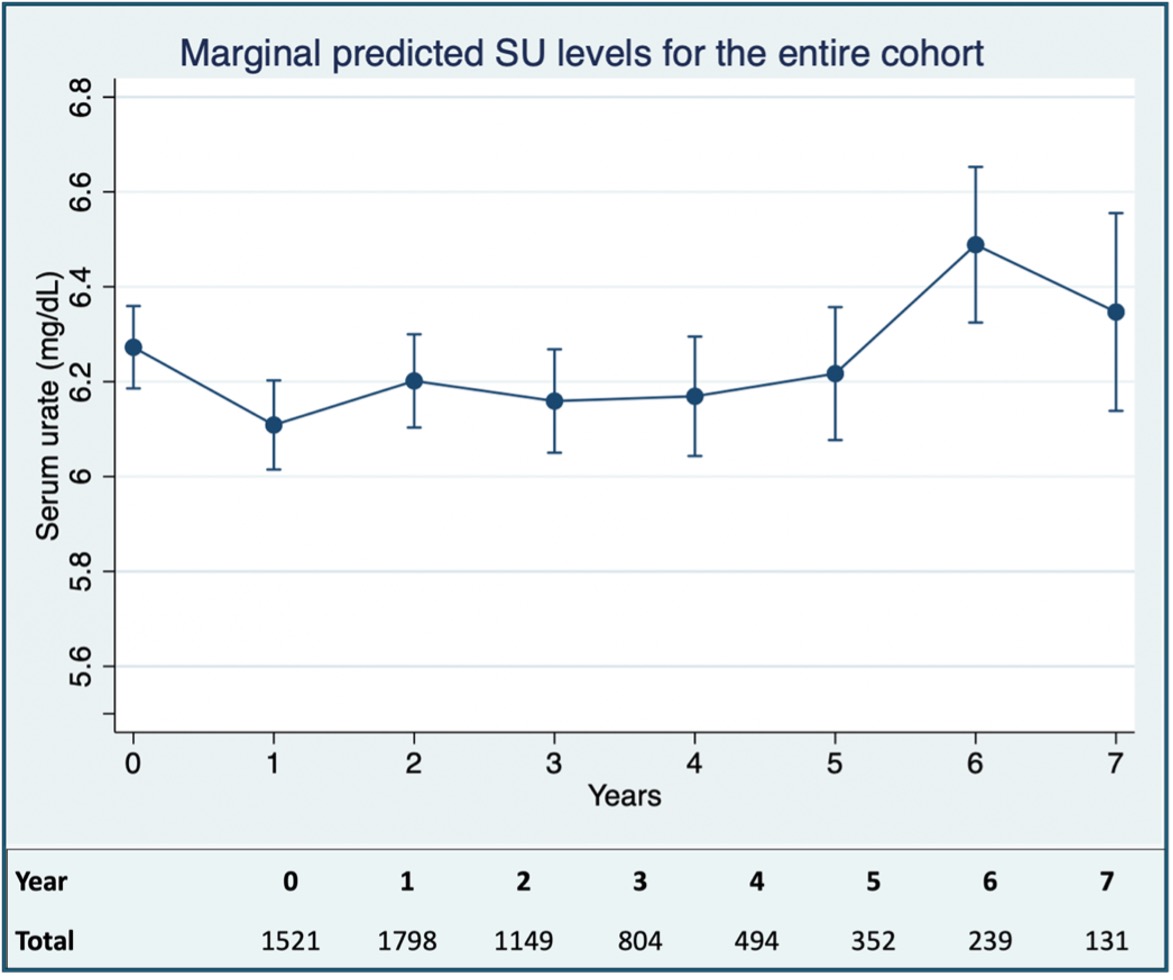
Results: Out of 25,526 individuals with prediabetes, 1,521 met the SU cohort requirements, contributing to 6,832 SU observations. At baseline, median age was 63 years and 40% were female. Median values were SU 6.3 mg/dL, HbA1c 5.9% and BMI 30 kg/m2. Medication use included aspirin (8%), losartan (2%), and diuretics (8%). Regarding comorbid conditions, hypertension was present in 33% of the patients, dyslipidemia in 21%, and chronic kidney disease in 5%.
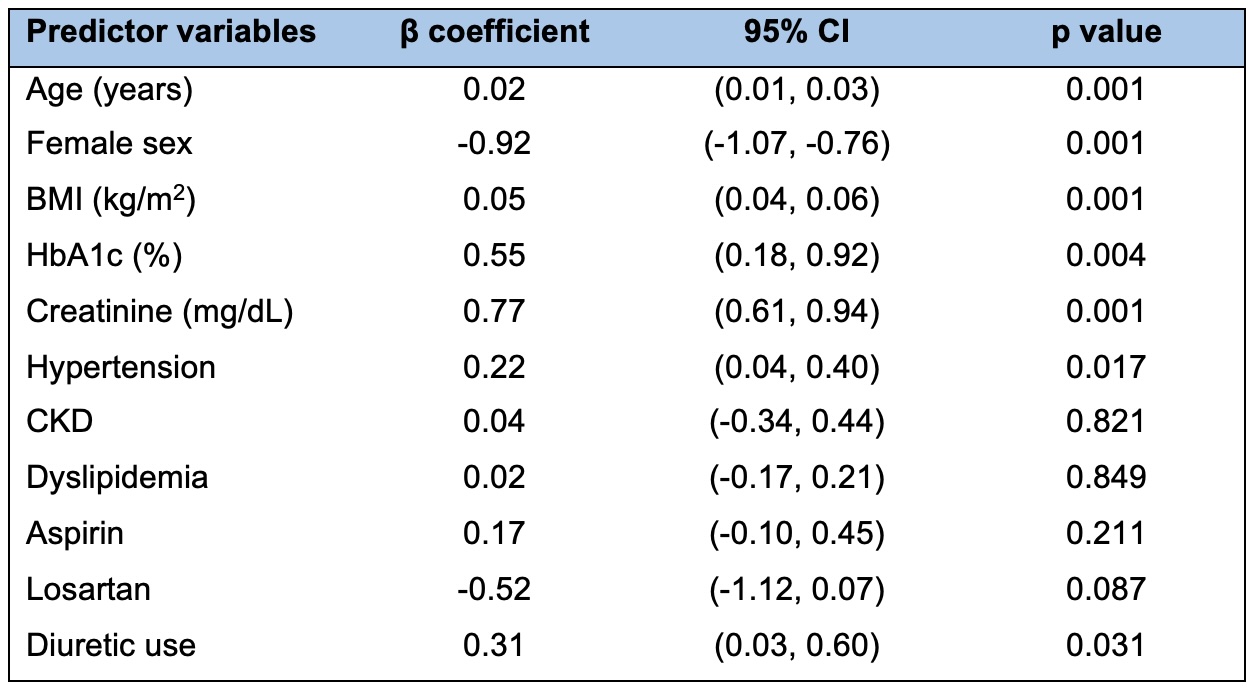
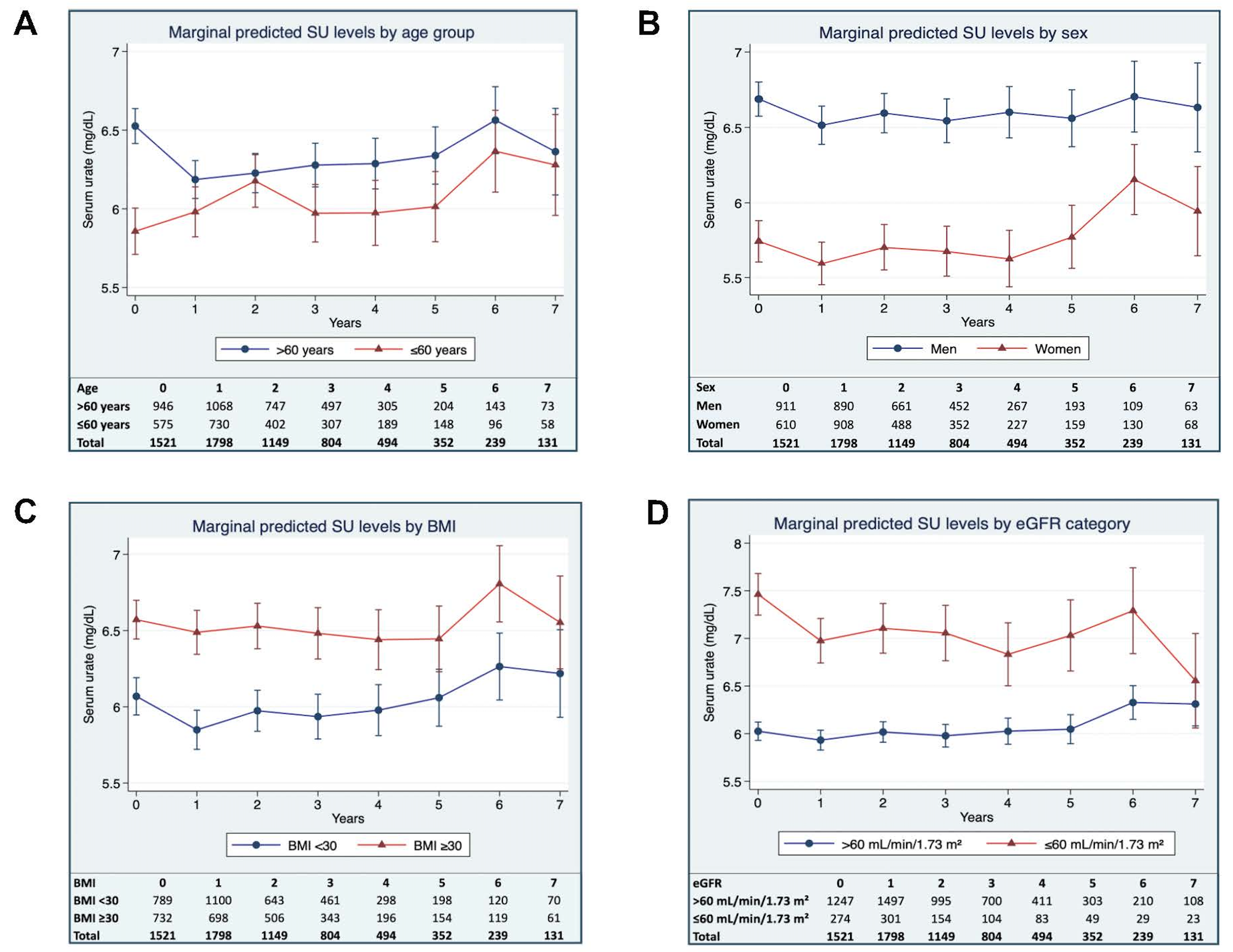
In general, mean SU levels increased during the study follow-up (Figure 1). Older age, male sex, greater BMI, and higher HbA1c were significant predictors of increased longitudinal SU levels (Table 1). In subgroup analyses, individuals aged ≤60 years consistently had lower SU levels compared to those >60 years (β = -0.66; 95% CI: -0.85, -0.48; p < 0.001). Similarly, females had lower SU levels than males, with an effect size of -0.94 mg/dL (β = -0.94; 95% CI: -1.12, -0.76; p < 0.001). Adults with a BMI ≥30 kg/m2 presented higher SU levels than those with a BMI < 30 kg/m2, with a 0.50 mg/dL increase in SU levels for each unit increase in BMI (β = 0.50; 95% CI: 0.32, 0.68; p < 0.001). Individuals with HbA1c levels from 6.1% to 6.4% exhibited higher SU levels compared to those HbA1c from 5.7% to 6.0% (β = 0.24; 95% CI: 0.05, 0.43; p = 0.010) (Figure 2).
Conclusion: Among individuals with prediabetes, older age, male sex, greater BMI, and higher HbA1c were significant predictors of increased SU over time. These longitudinal trends in SU, support the potential for early intervention during the prediabetic phase, possibly reducing gout risk.
To cite this abstract in AMA style:
Marrugo J, Santacroce L, Paudel M, Fukui S, Tedeschi S, Solomon D. Longitudinal Analysis of Serum Urate in Prediabetic Phase [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/longitudinal-analysis-of-serum-urate-in-prediabetic-phase/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/longitudinal-analysis-of-serum-urate-in-prediabetic-phase/