Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Recognizing muscle breakdown as a potential cause of elevated transaminases is crucial in the primary care setting to facilitate early referral to rheumatology for the evaluation of idiopathic inflammatory myopathy (IIM). Our purpose was to investigate the prevalence of preceding transaminitis in patients diagnosed with IIM and assess the timing of creatine kinase (CK) levels checked following transaminase (aspartate & alanine aminotransferase) elevation.
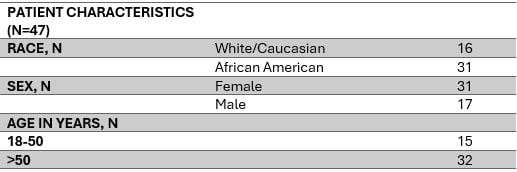
Methods: A retrospective chart review was conducted as a part of a quality improvement project to assess delays in diagnosis of IIIM using the electronic medical records of patients seen at the University South Carlina/Prisma Health Midlands rheumatology clinic between Jan 2021 and May 2024. Patients were included if they had relevant diagnosis codes (M60.9, G72.0, M33.2, M33.9, M60.80, D89.89, M33.10). Patient demographics including race, age, and sex were collected. Patients with a diagnosis of IIM but without evidence of muscle involvement were excluded. Muscle involvement was defined by having muscle-related symptoms and elevated CK levels. Charts were reviewed to collect levels of transaminases at the time of myositis diagnosis and up to 3 years prior. The duration between transaminases elevation and the first CK level checked were recorded. It was determined that abnormal transaminases were secondary to myositis if patients had no underlying liver disease and if the transaminase levels correlated with the CK levels with concurrent rise or fall.
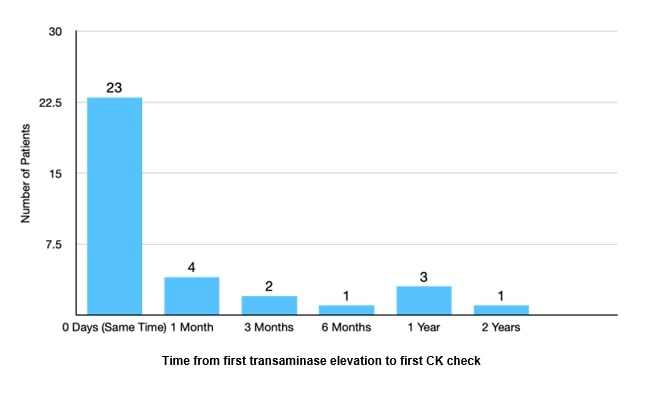
Results: A total of 140 patients with a diagnosis of IIM were identified. Of these, 47 patients were included in the study after excluding 93 patients without evidence of myopathy. 34 of the 47 (72%) had elevated transaminases either at the time of diagnosis or prior to the diagnosis of myositis/elevated CK. Out of the patients with elevated transaminases, 11 of the 34 (32%) experienced a delay in CK check, ranging from 1 month to just over 2 years. The patients were diagnosed with various types of myopathies: Anti-synthetase syndrome (17 patients), Connective tissue disease associated myositis (11 patients), Statin-induced (6 patients), Necrotizing myositis with negative antibodies (6 patients), Neuromyopathy (1 patient), Cancer related myositis (1 patient), Sarcoid myopathy (1 patient) and Dermatomyositis (4 patients). Common complaints before diagnosis included muscle weakness (66%), myalgias (30%) with less common symptoms being shortness of breath, arthralgias, and nonspecific extremity pain or heaviness.
Conclusion: Most patients diagnosed with myositis in our study had elevated transaminases, with a significant proportion showing persistently elevated AST/ALT prior to an elevated CK, suggesting the importance of considering transaminitis as an early indicator of IIM in patients without liver disease. We are implementing future interventions within the electronic medical record at Prisma health midlands to prompt primary care providers to check CK in patients with persistent unexplained transaminitis which will expedite diagnosis and improve patient outcomes.
To cite this abstract in AMA style:
nidhaan A, Iriza S, West A, martin M, Pethe G. Early Recognition of Myositis: Time Correlation Between Transaminases and Inflammatory Myopathy in a Community-Based Rheumatology Practice [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/early-recognition-of-myositis-time-correlation-between-transaminases-and-inflammatory-myopathy-in-a-community-based-rheumatology-practice/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/early-recognition-of-myositis-time-correlation-between-transaminases-and-inflammatory-myopathy-in-a-community-based-rheumatology-practice/