Session Information
Date: Saturday, November 16, 2024
Title: Abstracts: Miscellaneous Rheumatic & Inflammatory Diseases I
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Immunosuppressive therapy, including Tumor necrosis factor inhibitors (TNFi), is commonly used in the treatment of various inflammatory conditions, including extracardiac sarcoidosis. However, the use of these medications in cardiac sarcoidosis (CS) is limited due to prior evidence suggesting an association with worsening heart failure and other adverse cardiac events. This research aims to explore and clarify the link between TNFi therapy and heart failure in individuals with cardiac sarcoidosis.
Methods: This is a nationwide, retrospective study. We used the global, multicenter research network (TriNetX) database from 89 large healthcare organizations across multiple countries. We included patients over 18 years with a diagnosis of CS between January 1, 2014, and June 9, 2024, using ICD-10 and ICD-9 codes. Patients were compared based on the use of TNFi (infliximab, etanercept, golimumab, adalimumab or certolizumab pegol) using 1:1 propensity score matching. Matching accounted for demographics (age at diagnosis, race and gender), chronic associated comorbidities, immunosuppressant use and laboratory values at baseline. Outcomes included heart failure (HF), all-cause mortality, and arrhythmias. Exposure for outcomes was anytime post-index diagnosis, excluding patients with pre-index event outcomes, endocarditis and chronic ischemic heart disease. Risks ratios (RR) with 95% confidence intervals were calculated for each outcome, with a p-value < 0.05 considered significant.
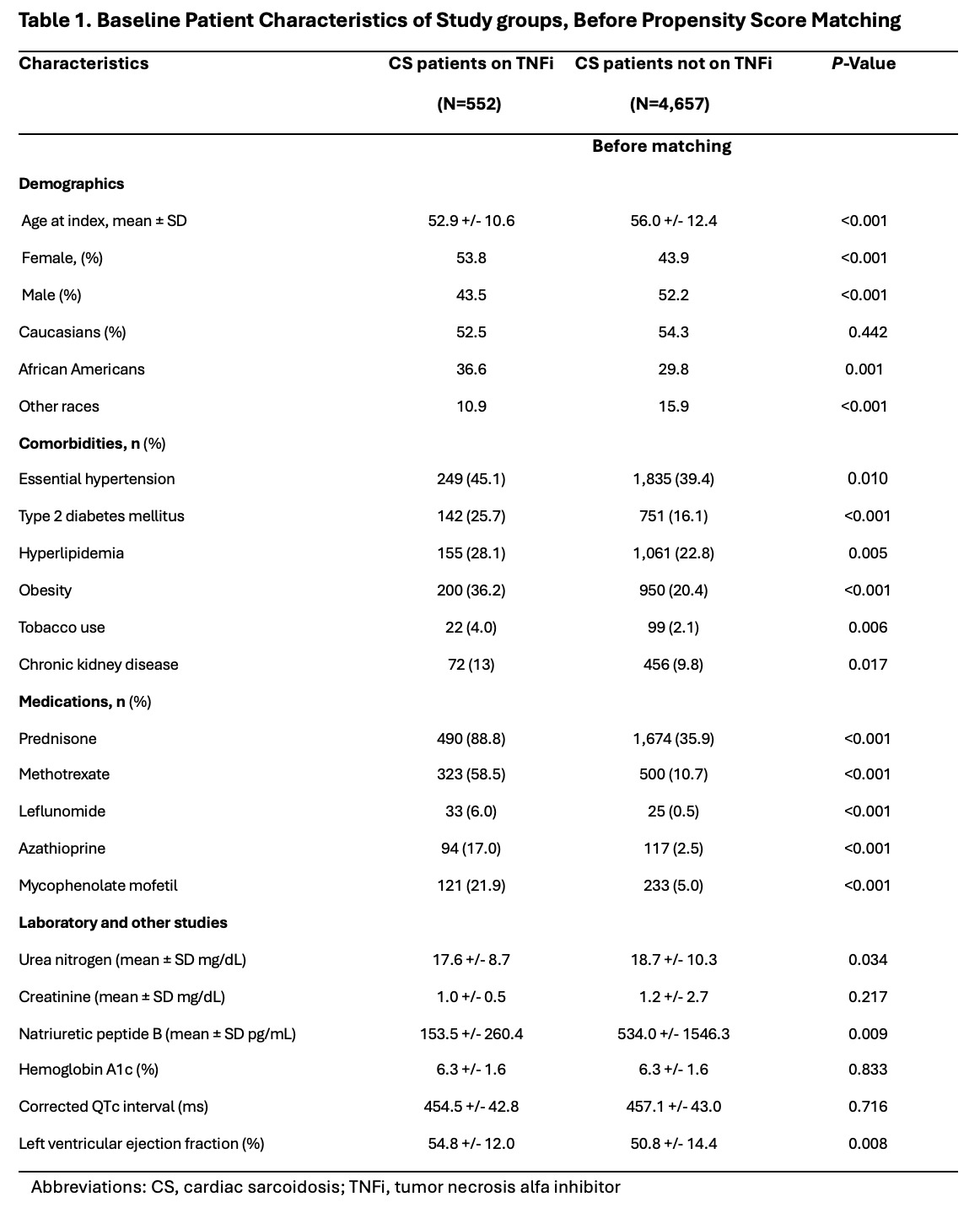
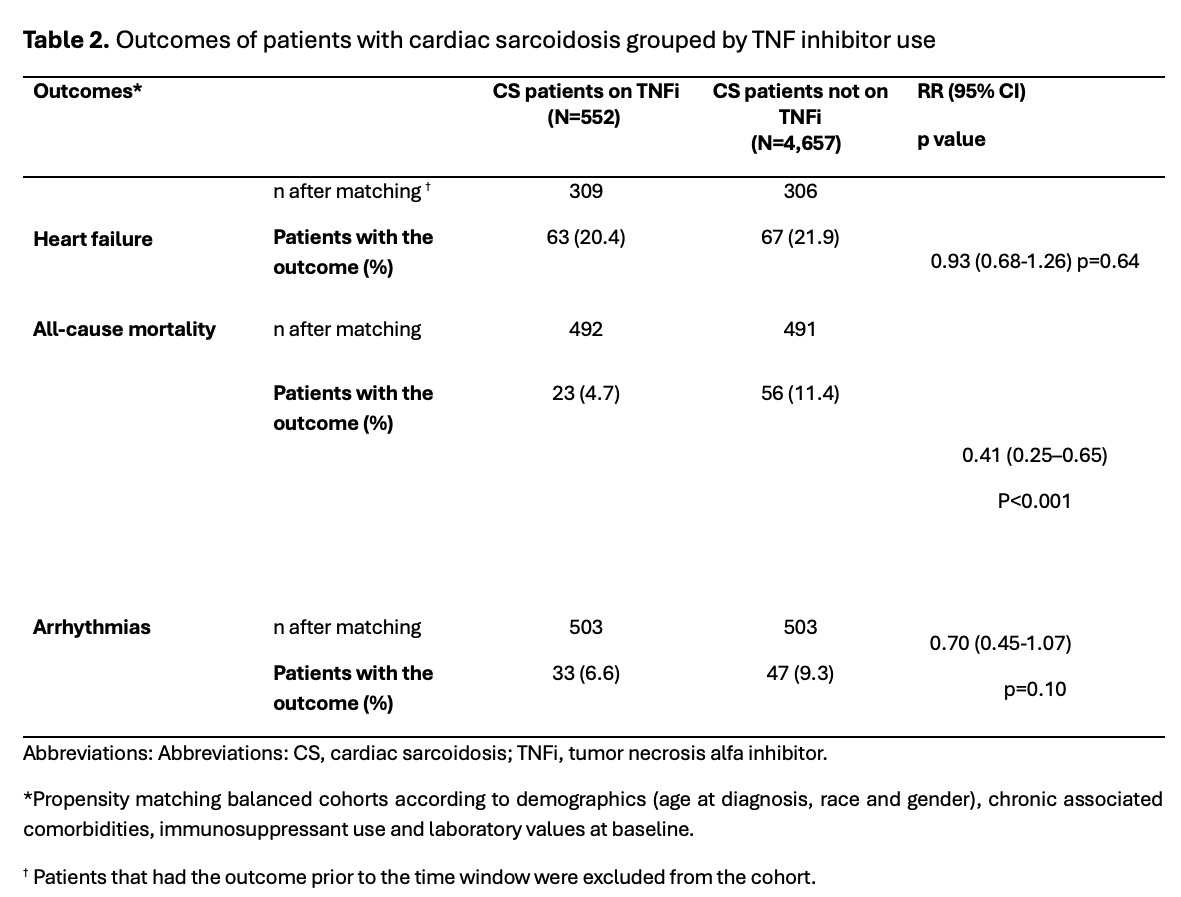
Results: We identified 552 patients with CS on TNFi and 4,657 patients with CS not on TNFi. Mean age at diagnosis was 52.9 ± 10.6 years for patients on TNFi and 56.0 ± 12.4 years for patients not on TNFi. CS patients on TNFi were more commonly females (53.8) while CS patients not on TNFi were more frequently males (52.2%). Likewise, Caucasians were the predominant race in both groups (52.5 and 54.3%, respectively). Comorbidities like (hypertension, type 2 diabetes, obesity, hyperlipidemia, tobacco use, and chronic kidney disease) as well as use of immunosuppressant medications were more common in CS patients on TNFi. Conversely, CS patients not on TNFi, had higher levels of urea nitrogen (18.7 +/- 10.3 vs 17.6 +/- 8.7 mg/dL, p=0.03) and natriuretic peptide B (BNP) (534.0 +/- 1546.3 vs 153.5 +/- 260.4 pg/mL, p=0.009) as well as a lower left ventricular ejection fraction (50.8 +/- 14.4 vs 54.8 +/- 12.0 %, p=0.008) when compared with patients on TNFi at baseline (See Table 1). After matching, CS patients on TFNi had a lower all-cause mortality risk (RR=0.41, CI95% 0.25-0.65; p< 0.001) compared to CS patients not on TNFi. No significant risk difference was found in HF and arrythmias outcomes between groups.
Conclusion: CS patients on TNFi have a lower all-cause mortality risk when compared with patients not on TNFi, without serious adverse effects including HF or development of arrythmias. Patients on TNFi also had lower urea nitrogen and BNP levels as well as a better LV function when compared with patients not TNFi. Further research is needed to better understand the effects and mechanisms of these medications in patients with CS
To cite this abstract in AMA style:
Gonzalez Moret Y, Lema D, Rodriguez Quinonez F. Exploring Clinical Outcomes of Patients with Cardiac Sarcoidosis on TNF Inhibitors: A Nationwide Retrospective Cohort Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/exploring-clinical-outcomes-of-patients-with-cardiac-sarcoidosis-on-tnf-inhibitors-a-nationwide-retrospective-cohort-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/exploring-clinical-outcomes-of-patients-with-cardiac-sarcoidosis-on-tnf-inhibitors-a-nationwide-retrospective-cohort-study/