Session Information
Date: Wednesday, November 15, 2023
Title: Abstracts: SLE – Diagnosis, Manifestations, & Outcomes IV: Outcomes & Comorbidity
Session Type: Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: Frailty, conceptualized as an accumulation of deficits across multiple physiological systems, was first examined in SLE in 2017 using the Fried Frailty Phenotype criteria and showed associations with functional decline, cognitive impairment, and mortality. Frailty in SLE has since been measured with other methods, including the recently-developed Systemic Lupus International Coordinating Clinics (SLICC) Frailty Index. We examined the agreement between 3 frailty measurement methods and the associations of frailty by each measure with outcomes.
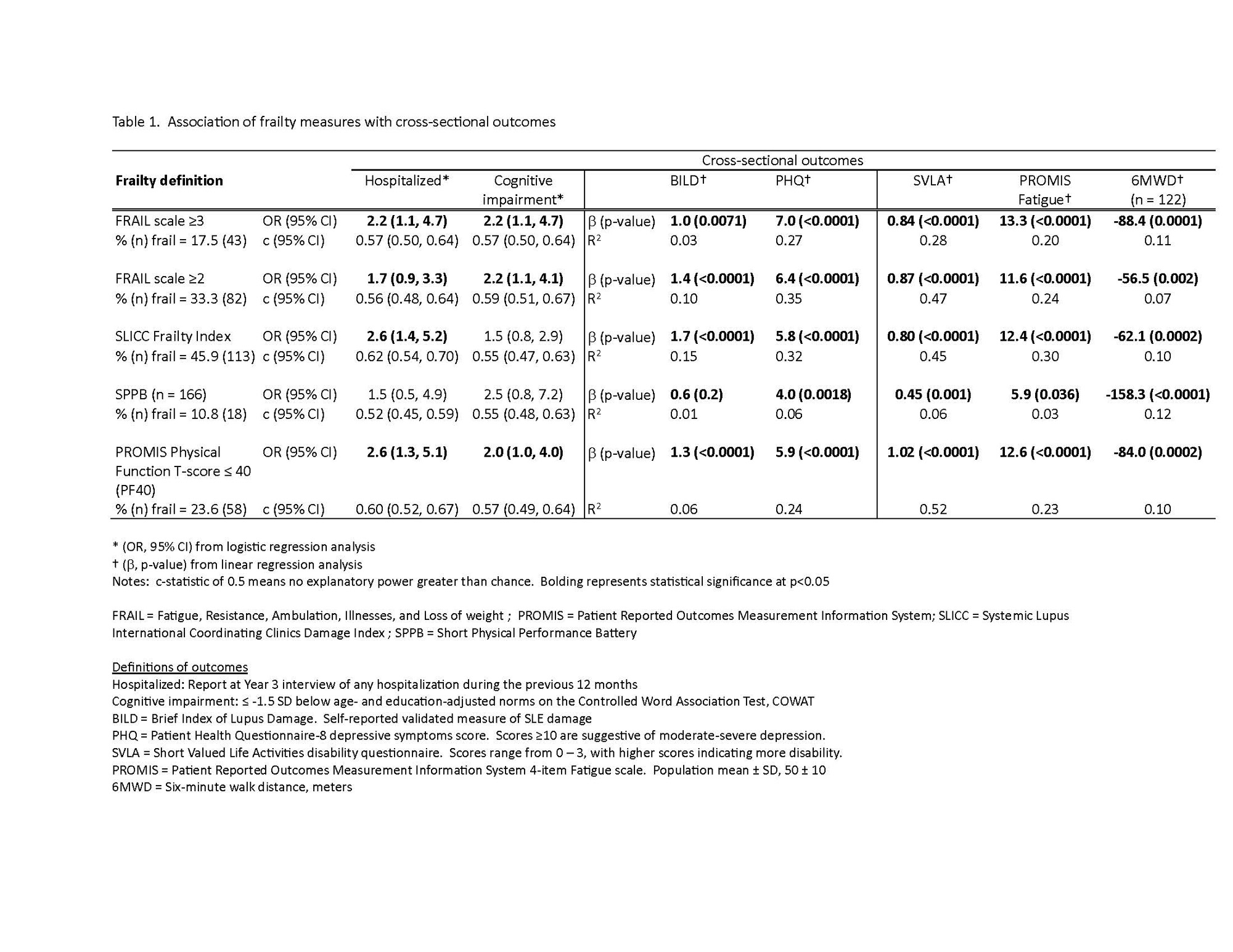
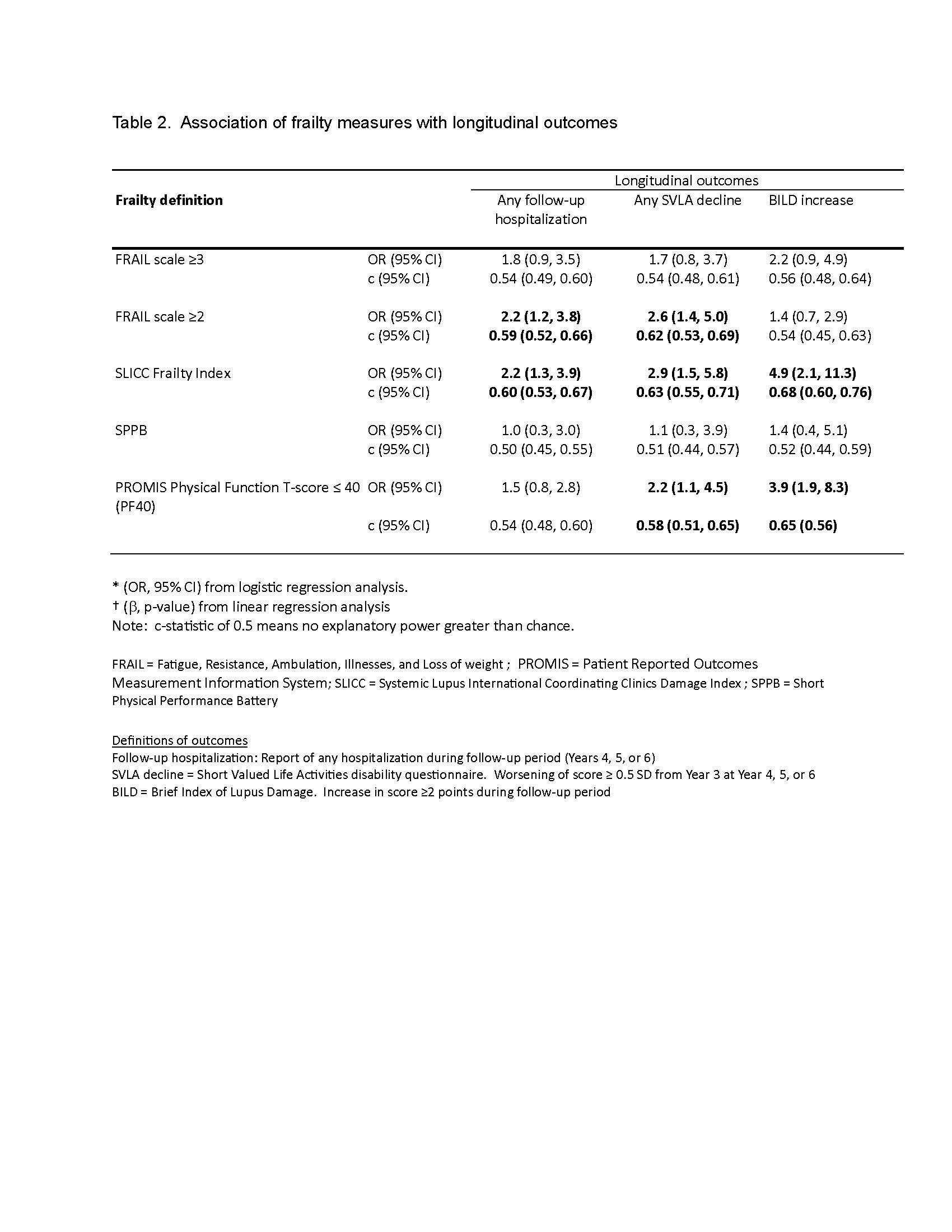
Methods: Data were from the California Lupus Epidemiology Study (CLUES), a longitudinal cohort with rheumatologist-confirmed SLE. Data are collected annually. In Year 3 (n=256), frailty was measured in 3 ways: SLICC Frailty Index (SLICC-FI), Short Physical Performance Battery (SPPB; n=166), and FRAIL scale (Figure 1). We also examined PROMIS Physical Function score ≤40 (1 SD below population mean) as a proxy for frailty (PF40). Kappa (k) analyses assessed agreement between frailty measures. Linear and logistic regressions examined cross-sectional associations between frailty and hospitalizations in the previous 12 months, cognitive impairment (≤ -1.5 SD below age- and education-adjusted norms on the Controlled Word Association Test, COWAT), distance walked in 6 minutes (6MWT), self-reported disease damage (Brief Index of Lupus Damage, BILD), disability (Short Valued Life Activities questionnaire, SVLA), fatigue (PROMIS Fatigue), and depressive symptoms (Patient Health Questionnaire, PHQ-8). Longitudinal outcomes examined were hospitalization, functional decline (SVLA score worsening ≥ 0.5 SD), and an increase in BILD ≥2 points at any point during the subsequent 3 years.
Results: Mean age was 48±14 years, SLE duration 19±11 years. The cohort was 90% female. Racial/ethnic representation was 37% Asian, 10% Black, 23% Hispanic, and 30% White (non-overlapping categories). Prevalence of frailty varied by measurement method: SLICC-FI, 45.9%; SPPB, 10.8%; FRAIL scale ≥3, 17.5%; FRAIL scale ≥2, 33.3%; PF40, 23.6%. Agreement among frailty measures was weak to moderate, with highest agreement between FRAIL≥2 and PF40 (k = 0.63), SLICC-FI and FRAIL≥2 (k = 0.62), and SLICC-FI and PF40 (k = 0.50). FRAIL≥3 and PF40 were significantly associated with all cross-sectional outcomes, FRAIL≥2 with all except hospitalization, SLICC-FI with all except cognitive impairment, and SPPB with SVLA, PHQ, 6MWD, and fatigue (Table 1). SLICC-FI was significantly associated with all longitudinal outcomes, FRAIL≥2 with follow-up hospitalizations and SVLA decline, and PF40 with SVLA decline and BILD increase (Table 2).
Conclusion: Agreement between measures of frailty in SLE is moderate at best. The SLICC-FI was a robust predictor of all SLE cross-sectional and longitudinal outcomes examined in this study except cognitive impairment. The simple FRAIL≥2 performed almost as well. The PROMIS PF, which may already be incorporated into many studies or clinical workflows, also performed well and may be used as a reasonable proxy for frailty. These data should inform selection of frailty measures for future studies in SLE.

To cite this abstract in AMA style:
Katz P, Dall'Era M, Barbour K, Greenlund K, Lanata C, Gordon C, Criswell L, Yazdany J. Measuring Frailty in SLE: Agreement Among Methods [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/measuring-frailty-in-sle-agreement-among-methods/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/measuring-frailty-in-sle-agreement-among-methods/