Session Information
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Rheumatoid Arthritis (RA) data indicate a “window of opportunity” during which DMARD therapy is most effective in achieving early and sustained remission, hence expedited access and early diagnosis is essential. Health status disparities exist in ethnic minority (EM) patients with rheumatic disease, inclusive of RA, particularly with early access and referral to specialty care. RA early referral tools have led to decreased wait times and increased numbers with the diagnosis. Therefore expedited referral in EM RA populations would be advantageous for early diagnosis and intervention. We evaluated a web-based referral tool developed to facilitate referrals of EM patients with symptoms of inflammatory arthritis to specialty care.
Methods: We designed an online referral tool, RHEUMATOID ARTHRITIS EARLY DIAGNOSTIC CLINIC [RAEDC], for primary care physicians (PCPs) at clinics serving EM patients. Based on the 4 domains of the ACR/EULAR 2010 RA Classification Criteria, the tool included a joint homunculus for PCP input of swollen and tender joints. PCPs received a RA educational lecture emphasizing the importance of early referral as well as joint exam techniques. Patients who received a score of ≥6 were scheduled for a RAEDC visit within 2 weeks. PCPs received feedback within 48 hours of the visit regarding RA diagnosis and accuracy of joint exam. Demographic data, RA disease status (Anti-CCP, RF), tender and swollen joint counts (TJC, SJC), ESR, CRP, and disease activity measures (RAPID-3, CDAI) were collected at baseline and compared to Ethnic Minority RA Consortium (EMRAC), an established disease cohort. Treatment patterns for the RAEDC cohort RA patients were assessed at baseline and at 3, 6, and 12 months. PCPs completed a 10-point Likert scale assessing utility of the referral tool.
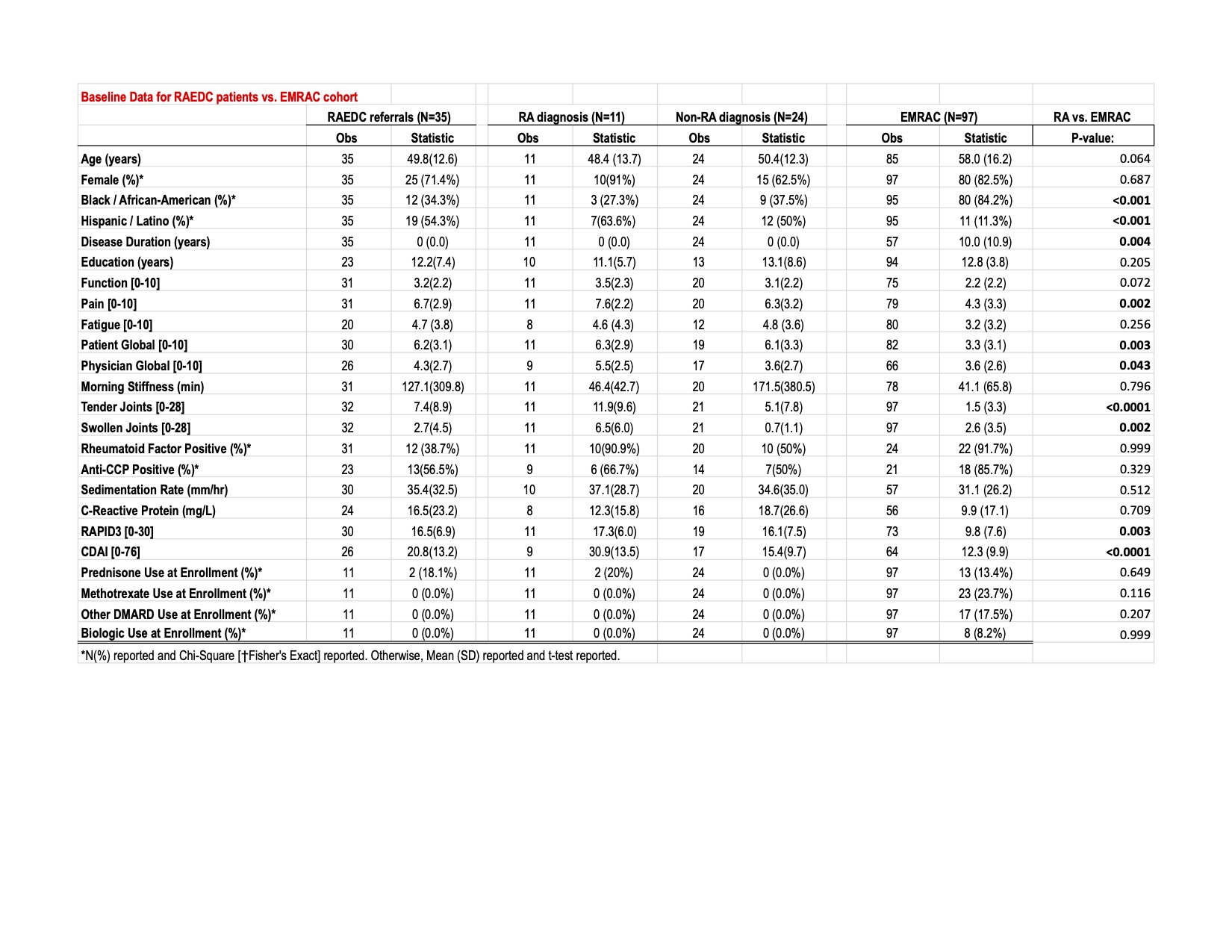
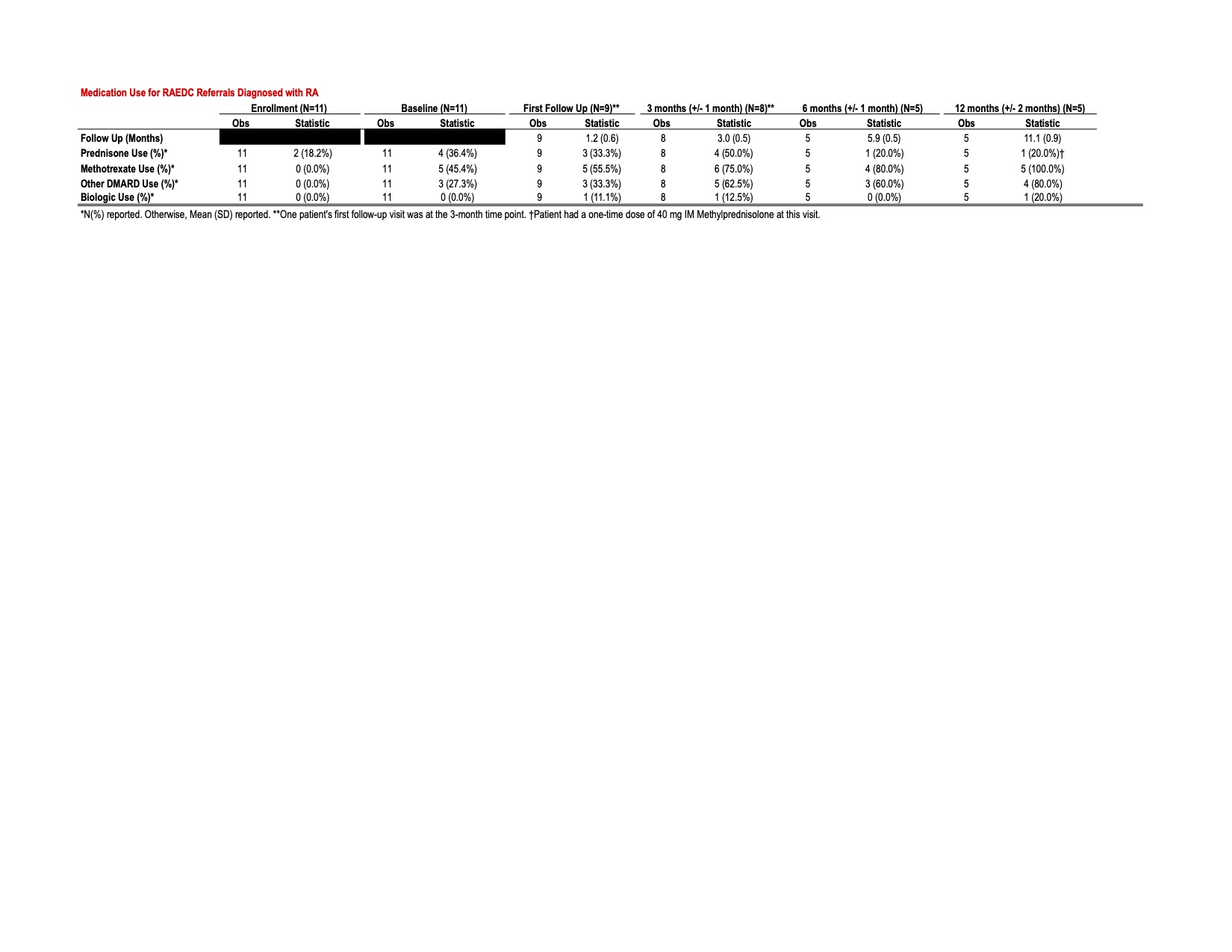
Results: Of 51 referrals, 35 were evaluated, and 16 did not keep their appointment. Of the 35 patients seen, 11 met ACR/EULAR RA Classification Criteria (31%). Whereas RAEDC patients were evaluated within 2-4 weeks of referral, the average time to diagnosis for the EMRAC cohort was 4 months. Compared to EMRAC, RAEDC patients were mostly Hispanic, with lower educational levels, higher pain/fatigue/patient global scores, TJC, SJC, ESR, CRP, and disease activity scores RAPID-3 (17.3 [6.0] vs. 9.8 [7.6], p=0.003) and CDAI (30.9 [13.5] vs. 12.3 [9.9], p < 0.0001) (Table 1). At initial visit, 72.7% received a DMARD (45.4% MTX, 27.3 % other DMARD), with 100% on a DMARD within a year (Table 2). Only 20% remained on Prednisone at 12 months. Alternate inflammatory diagnoses included Gout, PMR, and SS, despite ~50% of the referral cohort with a positive RA serology. PCPs indicated favorable utility of the online tool (Likert 7.8).
Conclusion: An online referral tool accompanied by initial teaching of PCP end-users served to increase RA awareness and early referral. The early access to specialty care led to initiation of DMARDs in all patients, with limited Prednisone use by one year. Our tool served to advocate for EM patients with low education status and emphasized the importance of joint exam by PCPs in the presence of RA serologies. Evaluations of improved accuracy in joint exam by PCPs and patient opinion in use of the online tool are planned.
To cite this abstract in AMA style:
Quinones M, Dowell S, Jileaeva I, Kadiri O, Swearingen C, Kerr G. Rheumatoid Arthritis Early Diagnostic Clinic: A Web-based Referral Tool Serving Ethnic Minority Patients [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/rheumatoid-arthritis-early-diagnostic-clinic-a-web-based-referral-tool-serving-ethnic-minority-patients/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheumatoid-arthritis-early-diagnostic-clinic-a-web-based-referral-tool-serving-ethnic-minority-patients/