Session Information
Date: Sunday, November 8, 2020
Title: RA – Diagnosis, Manifestations, & Outcomes Poster III: Cardiopulmonary Aspects
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Cardiovascular disease (CVD) is a leading cause of mortality in rheumatoid arthritis (RA). Ischemic heart disease in RA is often silent and precedes myocardial infarction. Patients’ understanding of conventional and RA-specific CVD risks is pivotal to improving CVD mortality in RA. We describe the results evaluating the effectiveness of a web based educational intervention (EI) for RA patients towards improving their CVD risk knowledge.
Methods: 296 consenting RA patients were enrolled through Rush University Rheumatology clinic. All patients completed demographics, Heart Disease Knowledge Questionnaire (HDKQ) and Heart Disease Fact Questionnaire-RA (HDFQ-RA)) at baseline; a higher score on the HDKQ & HDFQ indicates a higher level of knowledge. HDFQ-RA also includes RA specific CVD risk knowledge questions. An educational video was developed specifically for RA patients with emphasis on RA specific CVD risks. Patients in the EI arm (n=150) watched the 28-minute video, followed immediately by HDKQ and HDFQ-RA. All patients (EI and non EI) completed HDKQ and HDFQ-RA at a follow-up visit 3-4 months later. Medical chart reviews were completed for RA and CVD pertinent data. Correct response ratios (CRR) were obtained for both questionnaires. General linear model (GLM) analyses for repeated measure were used to compare within person changes with time and intervention status (EI or non EI) in CVD risk knowledge. Effect sizes (ES) for improvements were calculated.
Results: Mean age was 56.5±13.9 years, and 86% were women. 42% were Caucasians, and 40% were African American. There were no differences in EI or non EI group by age, gender, race, education, smoking, hypertension, dyslipidemia, diabetes, body mass index, disease activity or current use of steroids.
Mean (SD) CRR for HDKQ and HDFA-RA for 296 patients at baseline were 0.59 (0.18) and 0.76 (0.17) respectively. Summary scores for HDKQ and HDFA-RA at baseline, post intervention and 3 month follow up stratified by the study intervention group are shown in Table 1. Patients in the EI arm had significantly higher CRR on HDKQ than those in the non EI at baseline (p 0.007). Improvements in HDKQ were observed at 3 months in both EI (ES 0.35) and non EI (0.25) groups. Only within person changes in HDKQ were observed as significant on GLM. Large improvements were seen in the EI group on HDFQ-RA immediately post EI (ES 0.64), and the improvement in CVD risk knowledge was retained at 3 months post EI follow up (ES 0.48). There were no significant improvements noted in HDFQ-RA in non EI group patients at 3 months (ES 0.09). GLM showed both within (time) and between person changes (EI or non EI) to be significant with HDFQ-RA (Figure 1).
Conclusion: Large improvements in CVD risk knowledge (HDFA-RA) were observed among the patients who watched the educational intervention that specifically focused on RA related CVD risks, and the benefits were retained at 3 months. As expected, some improvements in CVD risk knowledge (HDKQ) were observed with time in both groups, as participation in the study and completion of the CVD risk questionnaires alone may have primed the participant’s interest in the topic.
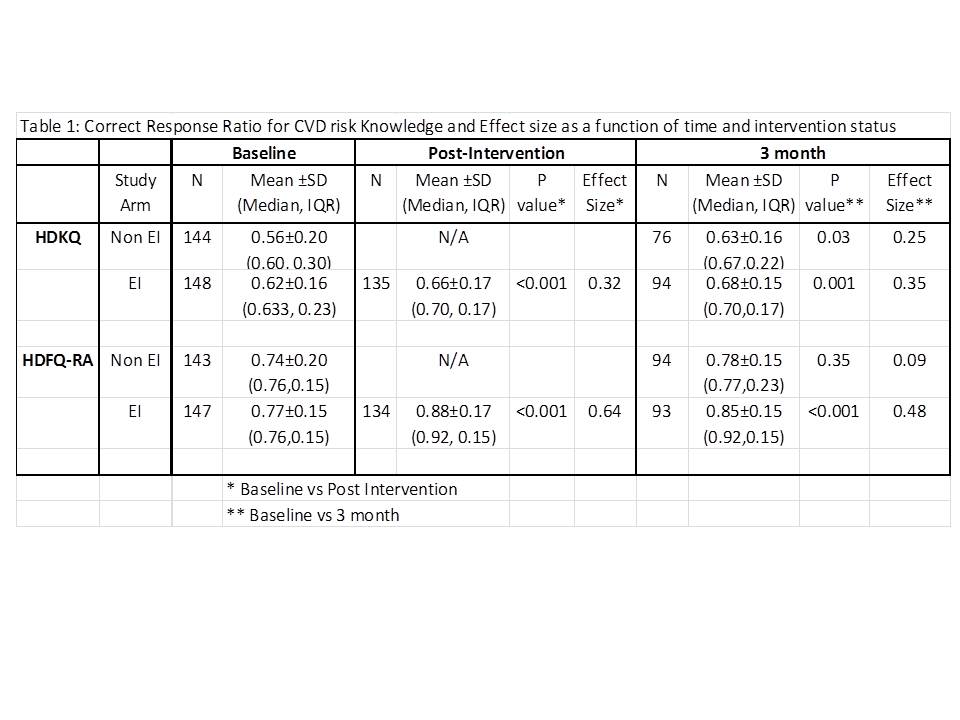 Table 1
Table 1
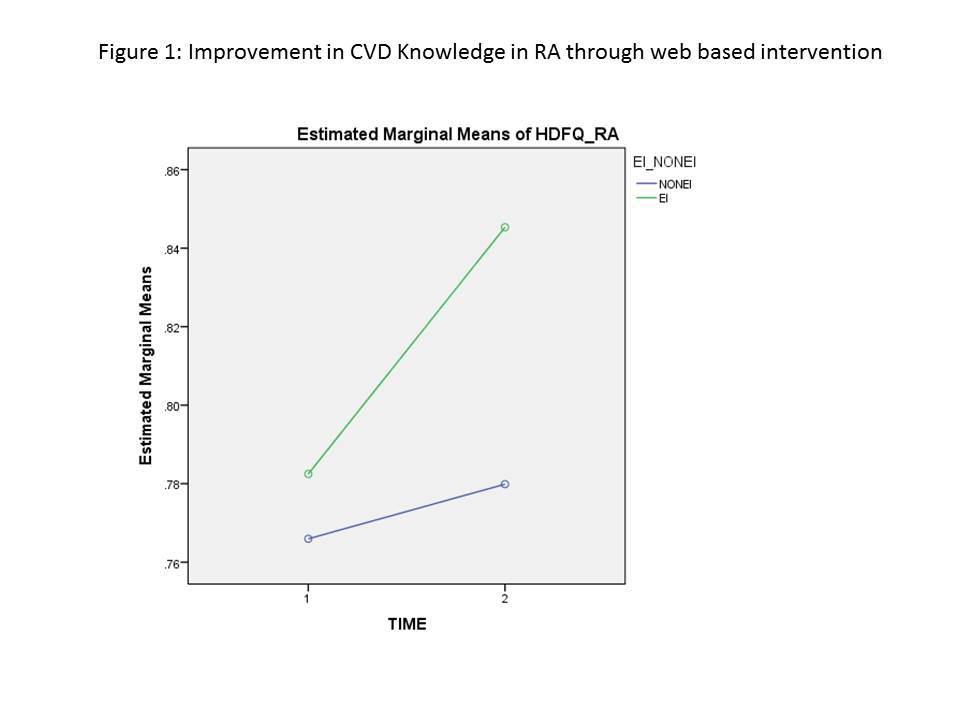 Figure 1
Figure 1
To cite this abstract in AMA style:
Jolly M, O'Brien C, Kugasia A, Gorfin A, Klebek L, Fair J, Block J. Gains in Cardiovascular Risk Knowledge Through Web Based Educational Intervention for Rheumatoid Arthritis Patients [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/gains-in-cardiovascular-risk-knowledge-through-web-based-educational-intervention-for-rheumatoid-arthritis-patients/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/gains-in-cardiovascular-risk-knowledge-through-web-based-educational-intervention-for-rheumatoid-arthritis-patients/