Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Knee osteoarthritis (KOA), particularly accelerated KOA, is associated with older age and being overweight. Greater age and weight are associated with impaired glucose homeostasis and elevated inflammation. There is a lot of interest in the role of glucose homeostasis and inflammation in KOA but it is unclear if they are associated with incident accelerated KOA. We aimed to determine if serum measures of impaired glucose homeostasis (glucose concentrations or glycated serum protein, GSP) or inflammation (high-sensitivity C-reactive protein, CRP) are related to incident KOA or incident accelerated KOA.
Methods: We conducted a case-control study using data from baseline and the first 4 annual visits of the Osteoarthritis Initiative. All participants had no radiographic KOA at baseline (Kellgren-Lawrence [KL] < 2). We classified 3 groups: 1) accelerated KOA: ≥ 1 knee progressed to advance-stage KOA (KL Grade 3 or 4) within 48 months, 2) typical onset of KOA: ≥ 1 knee increased in radiographic scoring within 48 months (excluding those with accelerated KOA), and 3) No KOA: no change in KL grade by 48-months. We did 1:1:1 matching based on sex. Weight-bearing, fixed flexion posterior-anterior knee radiographs were obtained at all visits. A laboratory blinded to group assignment conducted high-sensitivity singleplex assay for CRP (Aviscera Bioscience), colormetric/endpoint assay (GSP, MyBiosource), and glucose concentrations with deproteinized samples. Samples were tested in duplicate. Due to nonlinear relationships, we used 3 piece-wise multinomial logistic regression models to determine if baseline CRP, GSP, or glucose were associated with typical onset of KOA or incident accelerated KOA compared with no KOA. We adjusted for age, body mass index, and sex.
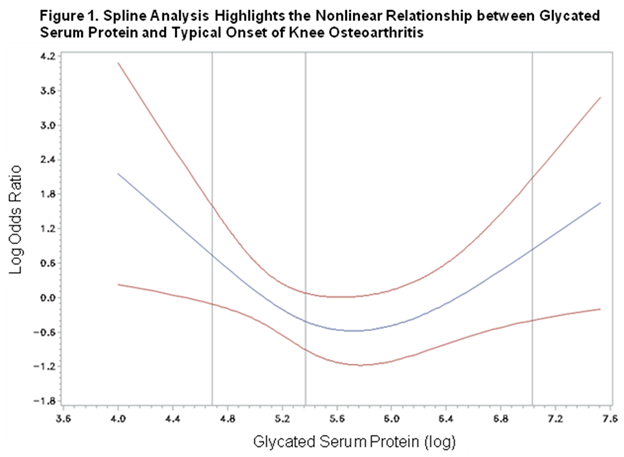
Results: We analyzed 54 adults/group and described their characteristics in Table 1. Baseline CRP, GSP, and glucose were not significantly associated with incident accelerated KOA (Table 2). However, lower and higher GSP concentrations were associated with a typical onset of KOA compared with adults with concentrations (log) closer to 5.4 (Table 2, Fig. 1).
Conclusion: Glucose homeostasis may predict individuals at risk of typical onset of KOA but not accelerated KOA. This is further evidence that accelerated KOA may be a distinct disorder from KOA.
| Table 1. No Significant Baseline Differences Among Those with Accelerated Knee Osteoarthritis (AKOA), Typical Onset of Knee Osteoarthritis (KOA), and no KOA | |||
| Baseline variable | No KOA (n = 54) | KOA (n = 54) | AKOA (n = 54) |
| Females (n, %) |
24 (63%) |
24 (63%) |
24 (63%) |
| Presence of Diabetes (n, %) |
1 (2%) |
0 (0%) |
4 (8%) |
| Age (years) |
59 (8) |
57 (8) |
62 (9) |
| Body Mass Index (kg/m2) |
27.3 (4.9) |
27.9 (4.6) |
28.9 (4.7) |
| Fasting Time (hrs) |
12 (2) |
12 (3) |
12 (2) |
| C-reactive Protein (mg/L) |
3.53 (1.09) |
3.16 (1.15) |
3.70 (1.05) |
| Glycated Serum Protein (ln) |
5.47 (0.58) |
5.51 (0.83) |
5.48 (0.77) |
| Glucose (mg/dL) |
111.25 (24.34) |
106.38 (24.90) |
107.27 (32.16) |
| Frequencies were analyzed with Chi-Square test and group means with paired-sample t-tests. | |||
| Table 2. Baseline Glycated Serum Protein Concentrations are Associated with a Typical Onset of Knee Osteoarthritis (KOA) | |||
| Predictor | No KOA | KOA (n=54) Adjusted OR | Accelerated KOA (n=54) Adjusted OR |
| C-Reactive Protein < 3.4 mg/L | REFERENCE | 0.70 (0.37,1.34) | 1.27 (0.58,2.79) |
| C-Reactive Protein > 3.4 mg/L | REFERENCE | 0.69 (0.33,1.45) | 0.91 (0.46,1.79) |
| Glycate Serum Protein (log) < 5.4 | REFERENCE | 0.14 (0.03,0.74) | 0.20 (0.04,1.09) |
| Glycate Serum Protein (log) > 5.4 | REFERENCE | 2.40 (1.02,5.63) | 1.78 (0.73,4.30) |
| Glucose <115 mg/dL | REFERENCE | 0.99 (0.97,1.02) | 0.98 (0.96,1.00) |
| Glucose >115 mg/dL | REFERENCE | 0.99 (0.95,1.03) | 1.02 (0.98,1.05) |
| All analyses are based on piece-wise regression models with cutpoints defined by graphing splines. All analyses are adjusted for age, body mass index, and sex (matching variable). There were no interactions with body mass index. | |||
To cite this abstract in AMA style:
Driban J, Eaton CB, Amin M, Stout A, Price LL, Lu B, Lo GH, McAlindon TE, Barbe M. Glucose Homeostasis Influences the Risk of Incident Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/glucose-homeostasis-influences-the-risk-of-incident-knee-osteoarthritis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/glucose-homeostasis-influences-the-risk-of-incident-knee-osteoarthritis/