Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Salivary gland ultrasound (SGUS) and minor salivary gland biopsy (MSGB) are widely used in the diagnosis of primary Sjögren’s syndrome (pSS). However, discordance between these modalities is frequently encountered, raising questions about their respective diagnostic value and the optimal strategy for resolving inconsistencies. This study aimed to investigate the prevalence and diagnostic relevance of discordance between SGUS and MSGB in pSS, and to evaluate whether Doppler ultrasound and histologic markers beyond the focus score provide additional diagnostic value in discordant cases.
Methods: Methods We retrospectively analyzed 128 patients (91 pSS, 37 non-pSS) who underwent both SGUS and MSGB within 12 months. SGUS was scored using the OMERACT system; grayscale ≥2 in at least one gland was defined as positive. Color Doppler signals were graded 0–3, and both total scores and a binary threshold (≥2 in any gland) were assessed. Patients were categorized into four groups: SGUS+/MSGB+ (Group 1), SGUS+/MSGB– (Group 2), SGUS–/MSGB+ (Group 3), and SGUS–/MSGB– (Group 4). MSGB was evaluated for focus score and additional histologic features (atrophy, fibrosis, ductal dilatation, lymphoepithelial lesions and germinal centers). The final diagnosis of pSS was determined by expert clinical judgment based on comprehensive evaluation, and served as the diagnostic gold standard for this study. Agreement between SGUS and MSGB was assessed using Cohen’s kappa. Logistic regression and ROC analysis were performed to evaluate the diagnostic value of Doppler in SGUS-negative patients and of extended histologic markers in MSGB-negative patients.
Results: Among the 128 patients, Group 1 included 51, Group 2 had 19 (13 pSS), Group 3 had 23 (22 pSS), and Group 4 had 35 (5 pSS). The overall discordance rate was 32.8%, and agreement between SGUS and MSGB was fair (κ = 0.334, p < 0.001). Among discordant cases, Group 3 (SGUS–/MSGB+) had a significantly higher pSS diagnosis rate than Group 2 (SGUS+/MSGB–) (95.7% vs. 68.4%, OR = 10.15, p = 0.034) (Figure 1), despite no significant differences in age, sex, USFR, or serologic status. In SGUS-negative patients (OMERACT grade 0–1), color Doppler signal showed a trend toward increased odds of pSS diagnosis (aOR = 1.57, p = 0.090), though its discriminatory power was limited (AUC ≈ 0.55). In the MSGB-negative subgroup (n=57), SGUS positivity (aOR = 1.51, p = 0.027) and fibrosis (aOR = 1.18, p = 0.040) were independently associated with pSS diagnosis and had the highest diagnostic performance (AUC = 0.666 and 0.621), whereas color Doppler signal and other extended histologic features showed limited diagnostic utility.
Conclusion: Diagnostic discordance between SGUS and MSGB is common in suspected pSS, with histologic positivity more strongly associated with diagnosis than SGUS findings alone. While OMERACT-based color Doppler ultrasound offered limited additional value in grayscale-negative patients, grayscale SGUS positivity and histologic fibrosis may help support the diagnosis in biopsy-negative cases. No significant clinical differences were found between discordant subgroups.
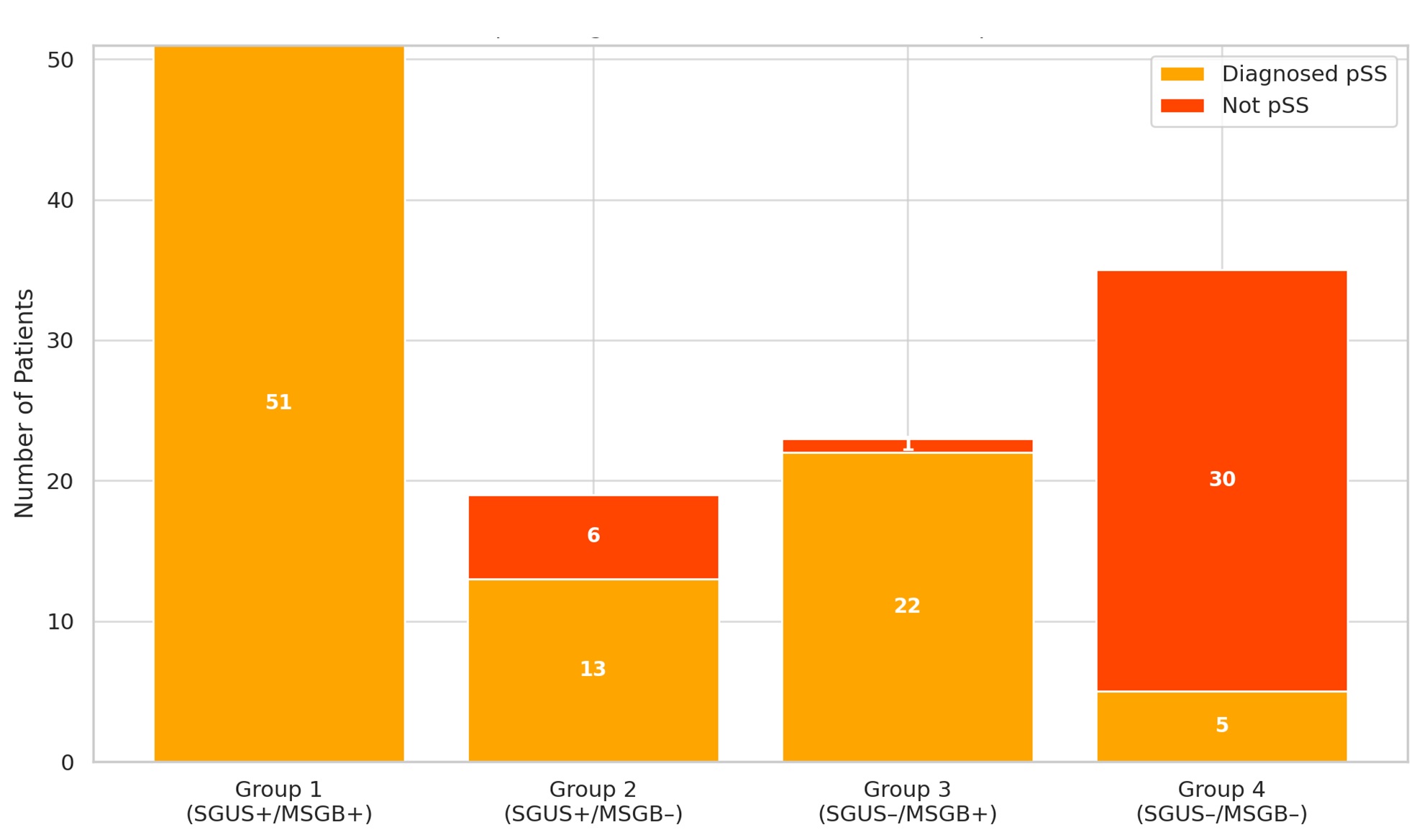
Figure 1. Diagnostic Distribution Across SGUS/MSGB Discordant Groups
Bar graph showing the number of patients diagnosed with primary Sjögren’s syndrome (pSS) versus not diagnosed, across discordant SGUS/MSGB groups.
Group 2: SGUS positive / MSGB negative
Group 3: SGUS negative / MSGB positive
Group 3 exhibited a significantly higher pSS diagnosis rate (95.7%) compared to Group 2 (68.4%), with an odds ratio (OR) of 10.18 (95% CI: 1.03–100.0, p = 0.047).
To cite this abstract in AMA style:
Lee k, Kim Y, Kim S, Kim H. When Imaging and Biopsy Disagree: Diagnostic Value of Doppler Ultrasound and Histologic Features beyond the Focus Score [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/when-imaging-and-biopsy-disagree-diagnostic-value-of-doppler-ultrasound-and-histologic-features-beyond-the-focus-score/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/when-imaging-and-biopsy-disagree-diagnostic-value-of-doppler-ultrasound-and-histologic-features-beyond-the-focus-score/