Session Information
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Change in radiographic joint space width (JSW) is used as a surrogate for cartilage loss and recognized by regulatory bodies as a measure of structural modification in DMOAD trials. However, both a reduction in cartilage thickness and meniscal integrity are inferred from a reduction in JSW. JSW measurement may be measured at any position in either the medial or lateral compartment. Often, the minimum JSW (minJSW) is measured because it is easily defined. However, the position of this minimum in the compartment can change between timepoints in a longitudinal study. Although the use of software can more reproducibly measure JSW at an arbitrary fixed position with greater sensitivity to change [1], the minJSW has persisted as a structural quantitative OA measure. More recently, minJSW has been used in the definition of Rapidly Progressing OA (RPOA1) in anti-NGF pharmaceutical trials.
We aimed to determine (i) the most common position for radiographic minJSW measurement in the medial compartment; (ii) the relative contributions of the average meniscal height and cartilage thickness at that position measured from 3D MR images; and (iii) how this compares to a fixed position medial JSW at the x=0.225 position [1] on a unit scale across the femur.
Methods: We used all 5,563 baseline knee images from the OAI that had minJSW measures to determine the median position of minJSW in the medial compartment for various Kellgren-Lawrence Grades (KLG) and OARSI JSN Grades. We performed careful manual segmentation of the meniscus and cartilage on a convenience set of 179 baseline OAI MRI DESS-we images, randomly chosen to provide representative samples of KL0/1, KL2 and KL3 grades. The medial tibial plateau of a mean 3D statistical shape model (SSM) of the knee was divided into 0.025-width anterior-posterior strips. These strips were projected from the mean SSM to each of the 179 3D knee examples and the relative contributions of meniscal height and cartilage to the total femur-tibia inter-bone distance were computed along each strip. A nearest strip was chosen to correspond with the median position of minJSW and compared with the strip at x=0.225.
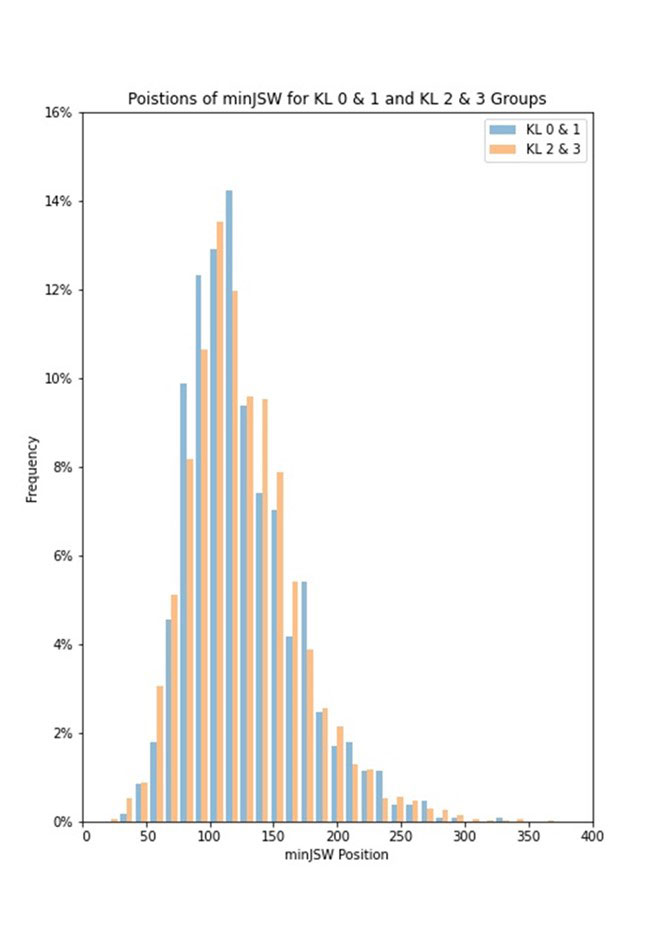
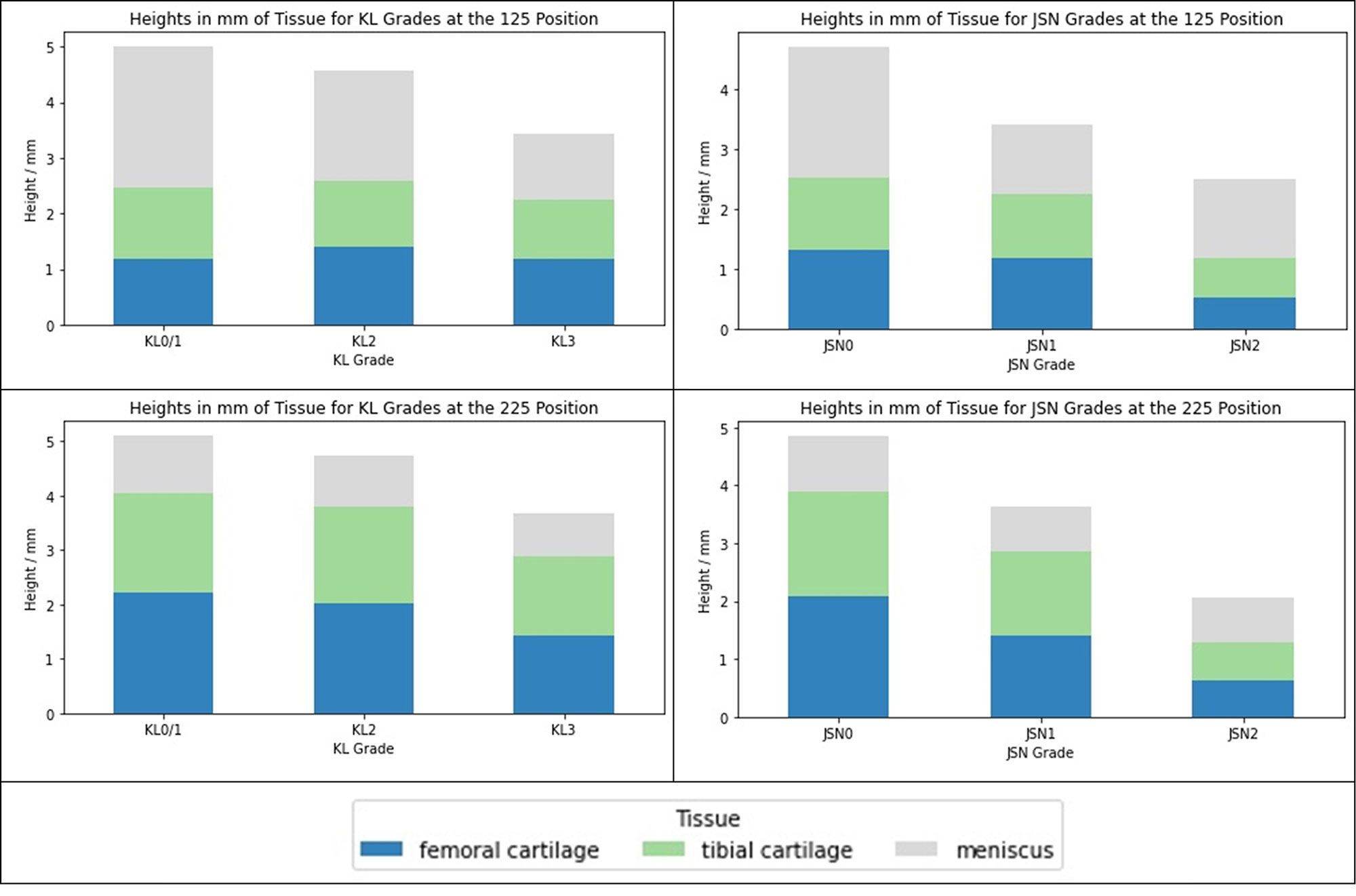
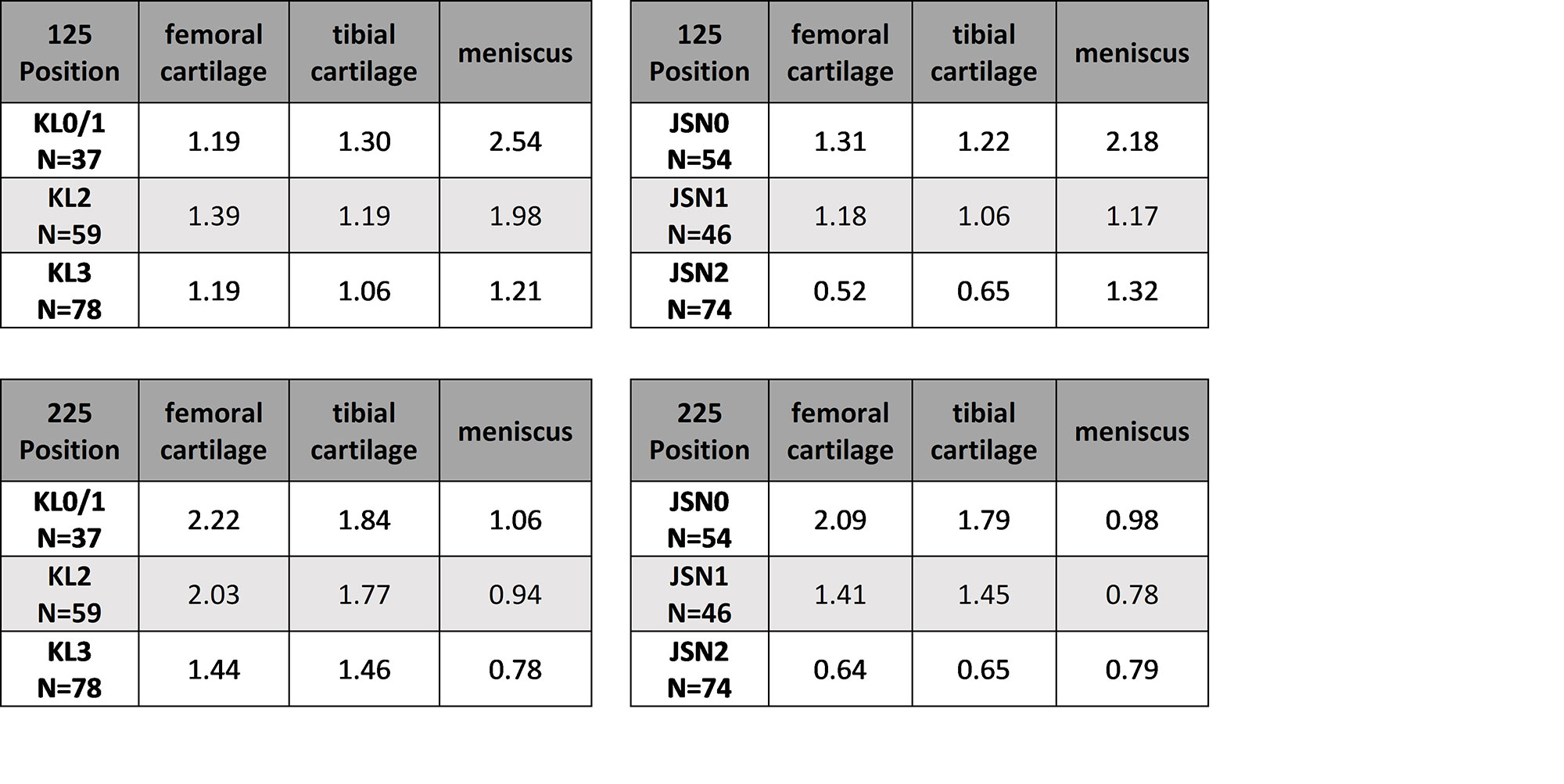
Results: Median medial compartment minJSW was found at the 0.119 position, this was consistent between KL0/1 and KL2/3 groups (Figure 1). The strip centered on x=0.125 was chosen to represent this position. Relative contributions of meniscus height and cartilage thickness to the inter-bone distance for the 0.125 and 0.225 positions are shown in Figure 2 and Table 1.
Conclusion: At the minJSW position (x=0.125), changes in meniscal height account for almost all of the differences between KLG and JSN groups, though cartilage does decrease significantly in the JSN2 group. At the 0.225 position, there is little difference in meniscal height at any stage of the disease, cartilage changes dominate the differences between all groups. While minJSW may be a useful measure of OA disease state, it is primarily a surrogate of meniscal and not cartilage changes, in contrast to the fixed position JSW measurements in the centre of the medial compartment, which better represents changes in the cartilage.
[1] Wirth, W. et al (2013). O&C 21(1), 117–125.
To cite this abstract in AMA style:
Brett A, Bowes M, Conaghan P. What Does Radiographic Minimum JSW Actually Measure? Comparison of Radiographic and MRI Measures Using Data from the OAI [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/what-does-radiographic-minimum-jsw-actually-measure-comparison-of-radiographic-and-mri-measures-using-data-from-the-oai/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/what-does-radiographic-minimum-jsw-actually-measure-comparison-of-radiographic-and-mri-measures-using-data-from-the-oai/