Session Information
Date: Friday, November 6, 2020
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster I: Clinical Manifestations
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: SLE is clinically heterogenous and its diagnosis is often difficult or delayed. The length of time from symptom onset or from when patients seek care for symptoms to SLE diagnosis has been reported to average 2-3 years. Early recognition and diagnosis provide the chance for timely treatment to minimize organ damage and improve outcomes. We aimed to develop predictive models for SLE diagnosis and to identify differences and overlap between early versus late predictors for SLE.
Methods: A case-control sample was created using the IBM MarketScan® Commercial Claims and Encounters database (2009-2019), which represents data from individuals enrolled in US employer-sponsored insurance health plans. Patients were classified as SLE cases if there were ≥3 outpatient diagnosis records (dx) that spanned at least 60 days, or ≥1 inpatient dx with ≥1 SLE medication records, or ≥1 SLE dx with ≥1 belimumab prescriptions. The first date of SLE dx code or belimumab prescription was designated as the index. Controls were 1:1 matched to each case by age, sex, and latest healthcare visit date (with any diagnosis) within 90 days of the case’ index date. All subjects were required to have ≥3 years of pre-index records with the 1.5-3 years and < 1.5 years pre-index periods defined as the early versus late time-window (Figure 1). A set of 171 candidate predictors from existing SLE classification criteria and the literature was observed in both time-windows and used to build 4 machine-learning models for each time window: regularized (L1) logistic regression, gradient boosted trees (GBT), XGBoost, and random forest. The models were trained and validated using 5-fold cross-validation in Dataiku DSS 5.0. Model performance was assessed by area under the receiver operating characteristic curve (AUC), accuracy and recall rate.
Results: A total of 13781 incident cases of SLE were identified and matched to the same number of controls. Mean age was 45 (median 47) years, and 87% were female. Table 1 describes the subjects’ characteristics: SLE cases had overall higher frequency of health care utilization (HU) than the controls, and generally higher frequency of HU in the late than the early time-window. Based on the same set of 171 candidate features, the top-performing machine learning model in the early and late time-windows was GBT, with AUC 0.82 and 0.90, accuracy 0.72 and 0.83, recall of 0.82 and 0.81, respectively. The other three models performed similarly. Predictors with the highest importance factor included blood metabolic panel, urinalysis, prescriptions for benzodiazepines, opioids and macrolides; and diagnoses of chronic pain, osteoarthritis, rheumatoid arthritis, and hypertension. The top 10 predictors for both windows were very similar (Table 2) though generally higher in frequency of occurrence in the late window (Table 1).
Conclusion: All 4 machine-learning models had good predictive performance, especially using predictors in late time-window. The set of predictors identified in the early window (1.5-3 years pre-index) overlapped substantially with that of the late window (< 1.5 years pre-index), indicating opportunities for earlier diagnosis.
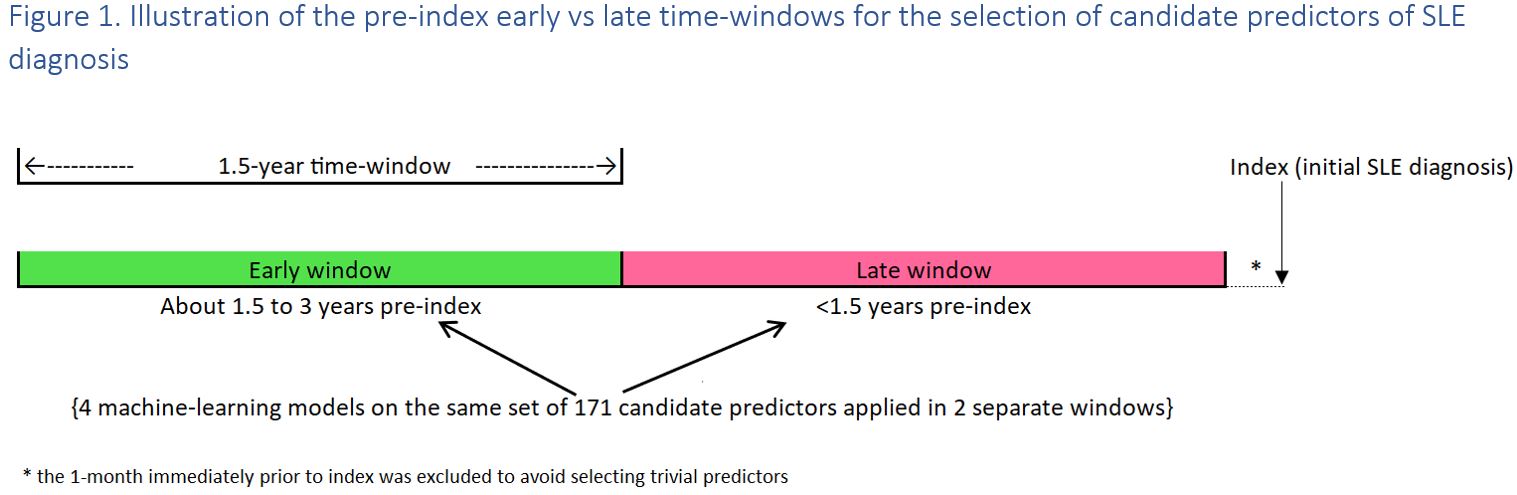
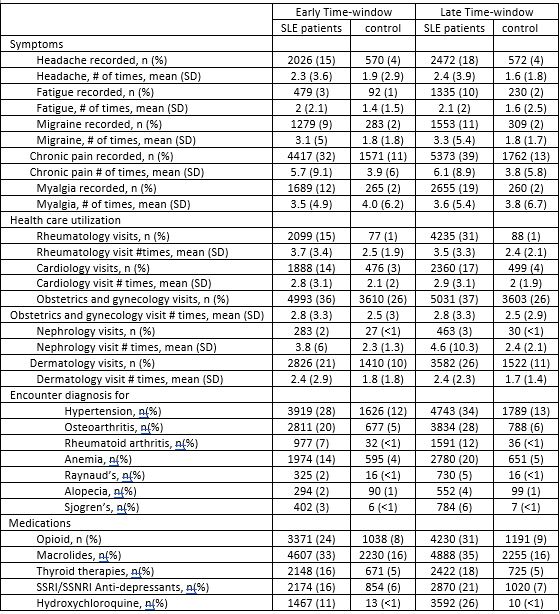 Table 1. Descriptions of the study populations, CCAE, 2009-2019 SSRI: Selective Serotonin Reuptake Inhibitors; SSNRI: selective serotonin-norepinephrine reuptake Inhibitors. Early Time-window: from index date- 1127 days to index-580 days; Late Time-window: from index-579 days to ~index-32 days
Table 1. Descriptions of the study populations, CCAE, 2009-2019 SSRI: Selective Serotonin Reuptake Inhibitors; SSNRI: selective serotonin-norepinephrine reuptake Inhibitors. Early Time-window: from index date- 1127 days to index-580 days; Late Time-window: from index-579 days to ~index-32 days
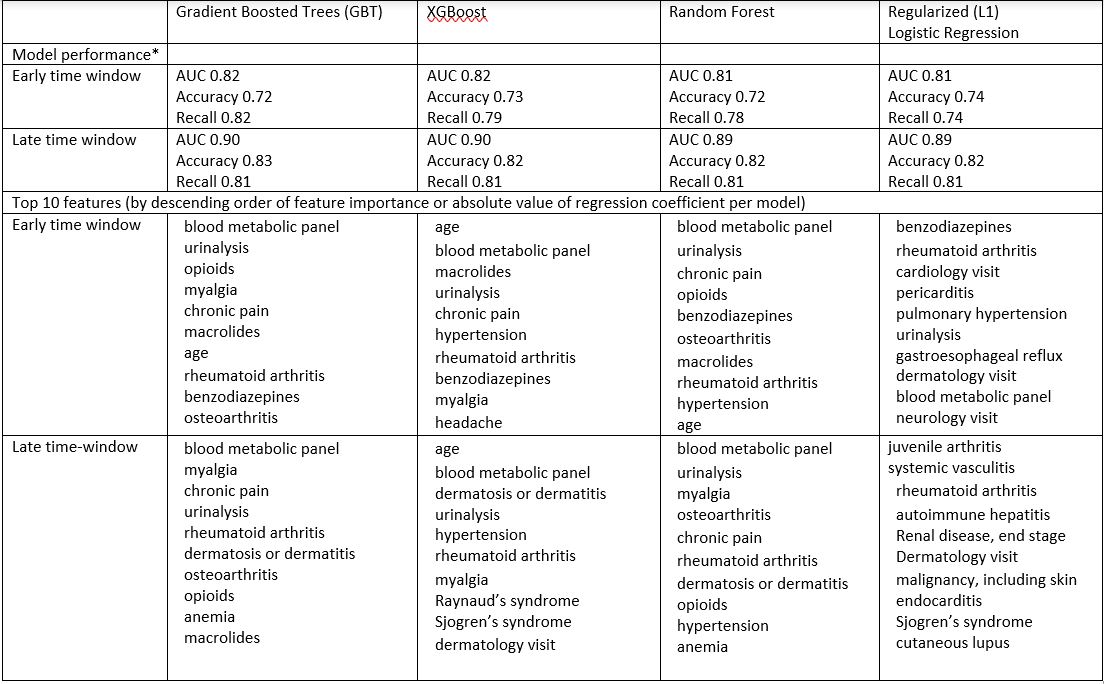 Table 2. Machine learning model results. *AUC: area under the receiver operating characteristic curve; accuracy: weighted arithmetic mean of positive predictive value (PPV) and Inverse PPV (weighted by Bias), where PPV was % true SLE case among those predicted as SLE case; recall: % of true SLE cases that were predicted as SLE case.
Table 2. Machine learning model results. *AUC: area under the receiver operating characteristic curve; accuracy: weighted arithmetic mean of positive predictive value (PPV) and Inverse PPV (weighted by Bias), where PPV was % true SLE case among those predicted as SLE case; recall: % of true SLE cases that were predicted as SLE case.
To cite this abstract in AMA style:
Wang Y, Lum K, Costenbader K, Wang G, Lofland J, Naessens D, Zhao Y, Davis K, Karyekar C. What Are the Early versus Late Predictors for Systemic Lupus Erythematosus (SLE) Diagnosis? [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/what-are-the-early-versus-late-predictors-for-systemic-lupus-erythematosus-sle-diagnosis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/what-are-the-early-versus-late-predictors-for-systemic-lupus-erythematosus-sle-diagnosis/