Session Information
Session Type: Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Rheumatoid arthritis (RA) is associated with accelerated atherosclerosis driven by chronic inflammation. We have previously reported that achieving sustained disease activity score 28 (DAS28) remission was associated with a significantly greater improvement in brachial-ankle pulse wave velocity (baPWV) in early RA (ERA) patients. This study was aimed to explore the long-term potential cardiovascular benefit of the well-recognized tight control treatment strategy in ERA. Whether treating to target over time is associated with long-term vascular outcomes in early RA (ERA) remained unclear.
Methods: This was a 5-year prospective study in patients with ERA. Consecutive ERA patients without overt cardiovascular disease were recruited. Patients received tight-control treatment in the first year, followed by standard-of-care management subsequently. Subclinical atherosclerosis was assessed using high-resolution carotid ultrasound (US) at baseline and year 5. The primary outcome was subclinical atherosclerosis progression (AP+), defined as incident plaque or an increased region harboring plaques, and/or maximum carotid intima-media thickness (max cIMT) progressed to over 0.9 mm at year 5. Disease activity score 28-erythrocyte sedimentation rate (DAS28-ESR) level was measured during each clinic visit. Cumulative averages of the area measured cumulative disease activity under the curve for DAS28-ESR (ca-DAS28-ESR) over a period of 5 years. Persistent LDA was defined as ca-DAS28-ESR ≤3.2.
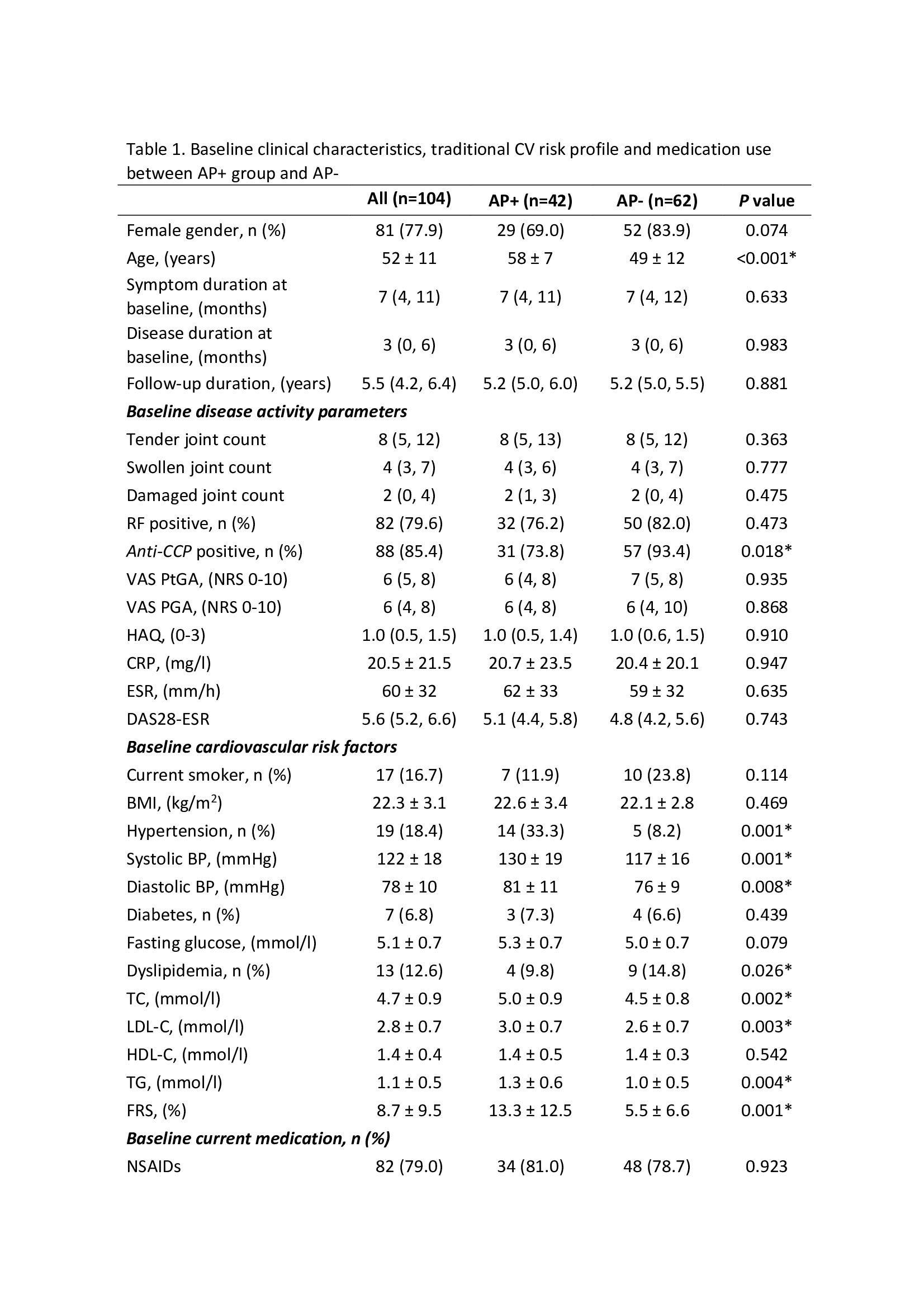
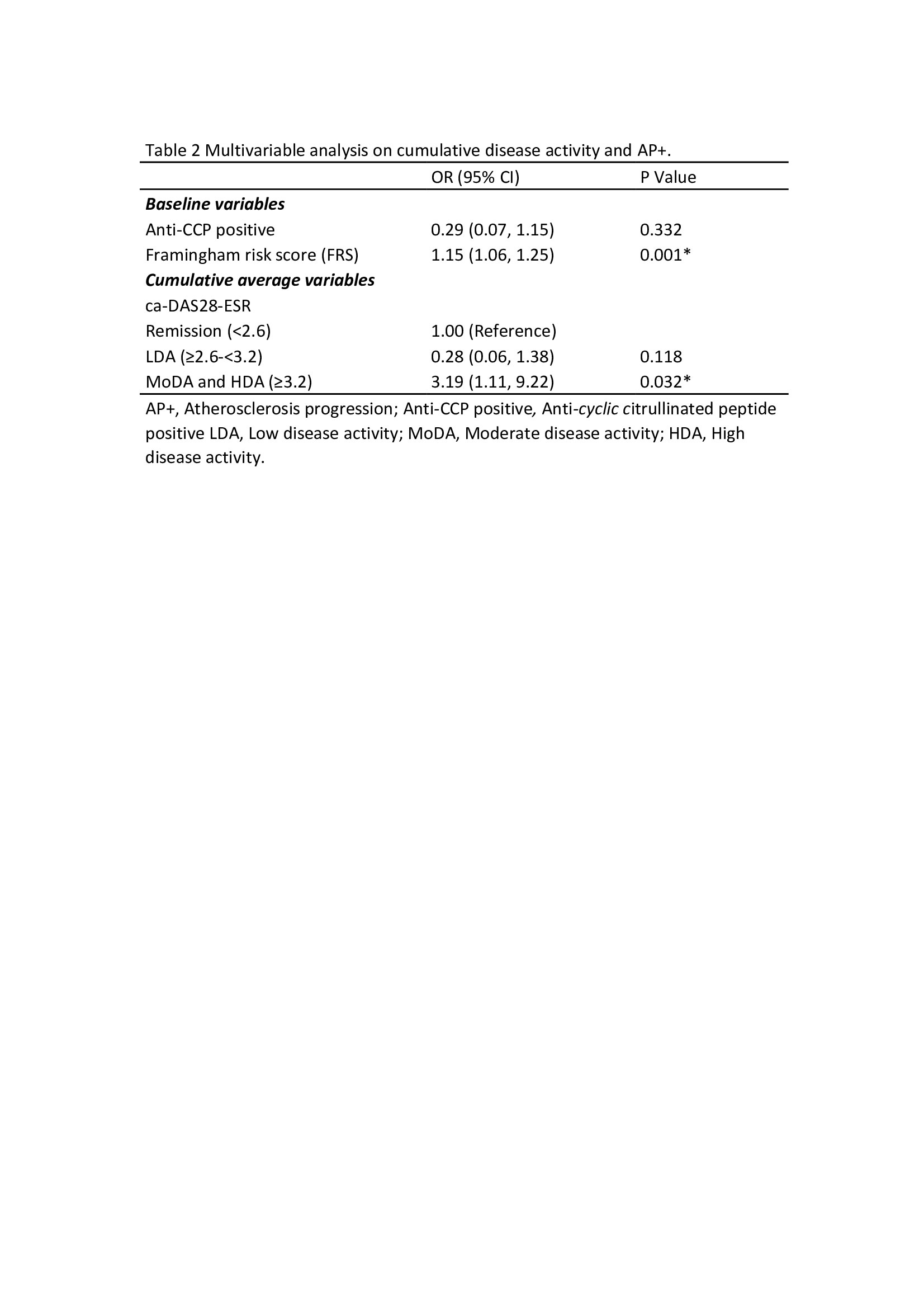
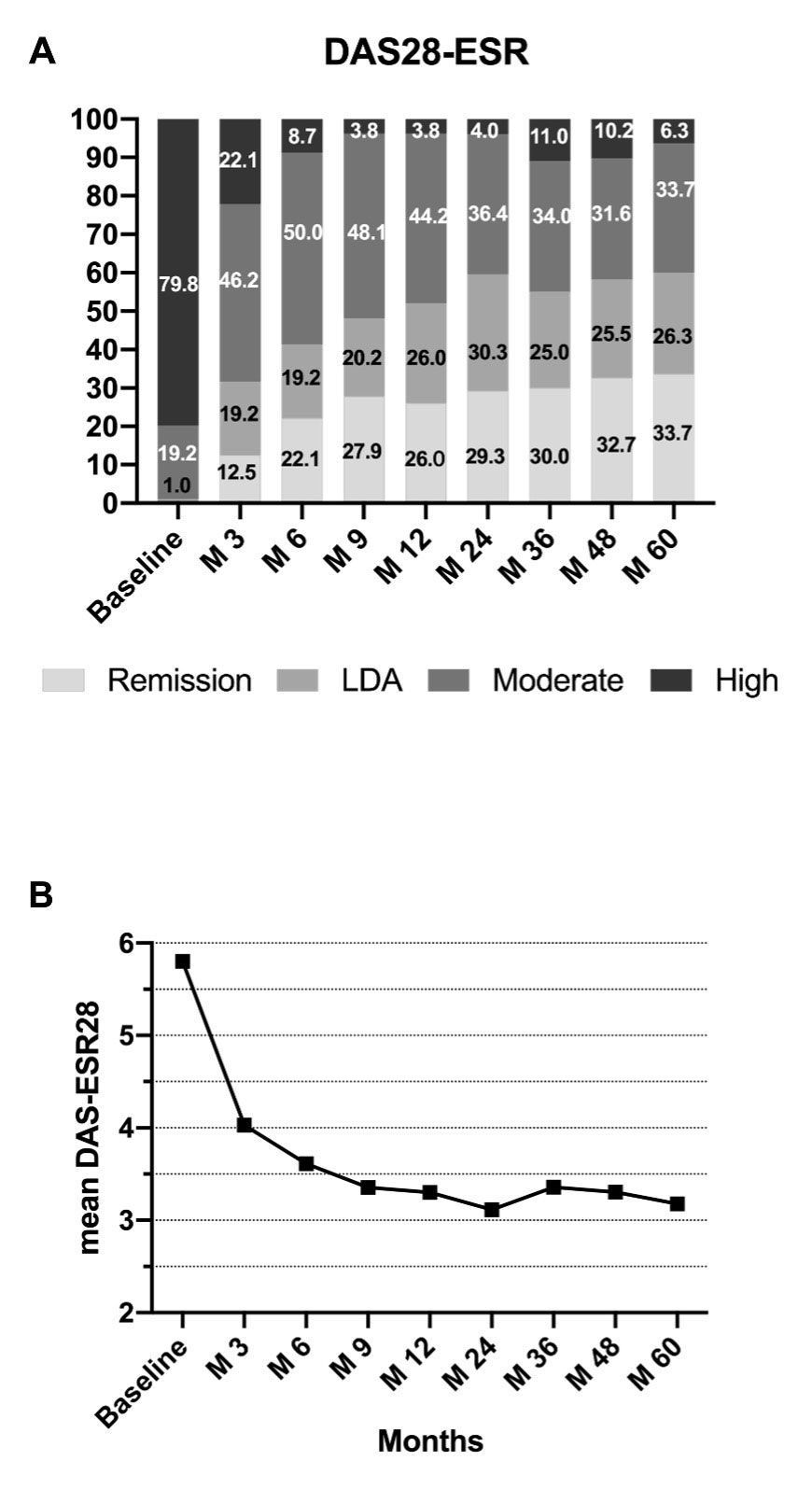
Results: One-hundred and four ERA patients (age: 52±11 years, 81(78%) female) who completed five years of follow-up were included in this analysis (Table 1). There was marked improvement in disease activity after five years of treatment (DAS-ESR at baseline: 5.8±0.9 vs. 3.2±1.2 at year 5, p< 0.001) (Figure 1). Fifty (47%) patients achieved persistent LDA. Forty-two patients (40.4%) had AP+. Patient in the AP+ group were older, had higher Framingham risk scores (FRS) and had higher exposure to anti-hypertension drugs at baseline (Table 1). The use of medication throughout study period was similar across two groups. In multivariate logistic regression, moderate and high disease activity was an independent predictor with AP+ (OR=3.19, 95% CI: 1.11-9.22, p=0.032) after adjustment for Anti-CCP positive and Framingham risk score at baseline (Table 2).
Conclusion: Achieving persistent LDA was an independent predictor of subclinical atherosclerosis in ERA. Effective long-term suppression of disease activity is required to minimize cardiovascular risk.
To cite this abstract in AMA style:
Meng H, Cheng I, Yan B, Lee A, So H, Tam L. Vascular Effect of Treat to Target in Early Rheumatoid Arthritis Patients – A 5-year Prospective Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/vascular-effect-of-treat-to-target-in-early-rheumatoid-arthritis-patients-a-5-year-prospective-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/vascular-effect-of-treat-to-target-in-early-rheumatoid-arthritis-patients-a-5-year-prospective-study/