Session Information
Date: Monday, November 8, 2021
Title: Epidemiology & Public Health Poster III: Other Rheumatic & Musculoskeletal Diseases (1022–1060)
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: Total Knee Arthroplasty (TKA) is an effective treatment option for end-stage knee osteoarthritis. The US is well known for having striking wealth-based disparities in healthcare access and outcomes. While it is assumed that disparities in the US are larger than in other countries, there are few population-based studies that directly compare wealth-based disparities in the US with other high income countries. Our objective was to examine the relationship between neighborhood income and TKA utilization and outcomes in the US and Canada.
Methods: We used population-based administrative data fromPennsylvania(PA), USA and Ontario(ON) Canada to identify all patients age >18 who were hospitalized for primary TKA between 2012 to 2018 using ICD-9/10 codes. We linked patient-level data from each jurisdiction to community median household income using zip code of residence. In each country we independently stratified patients into neighborhood income quintiles. The primary outcome of interest was age and sex standardized per capita utilization of TKA (per 10,000 population per year) for patients in each country stratified by income quintile. Secondary outcomes included 90-day mortality, 90-day readmission, and 1-year revision rates.
Results: We identified 161,244 primary TKAs in ON and 208,016 TKAs in PA (Table 1). TKA utilization per 10,000 population per-year was significantly higher in PA than ON (29.5 vs. 22.8, p < 0.001). Across all income groups, utilization rates were significantly higher in PA compared to ON (31.4 vs. 17.5, p < 0.001 in lowest income quintile; 37.5 vs. 22.8, p < 0.001 in highest income quintile). (Table 2). In both PA and ON, those in the highest income quintile, had significantly increased odds of 90-day mortality (aOR = 1.58 in PA, 1.47 in ON ) and 90-day readmission (aOR = 1.24in PA, 1.30 in ON) compared to lowest income quintile. For 1-year revision were only significant in PA (aOR = 1.44) (Figure 1)
Conclusion: The population-based utilization of TKA is higher in PA, USA compared to ON, Canada. We observed significantly lower rates of TKA for residents of lower income neighborhoods in both the US and Canada and the relative difference between low and high income communities is similar in both countries. In the context of the ongoing debate over healthcare reform in the US, our findings suggest that a single-payer system is unlikely to eliminate income-based disparities.
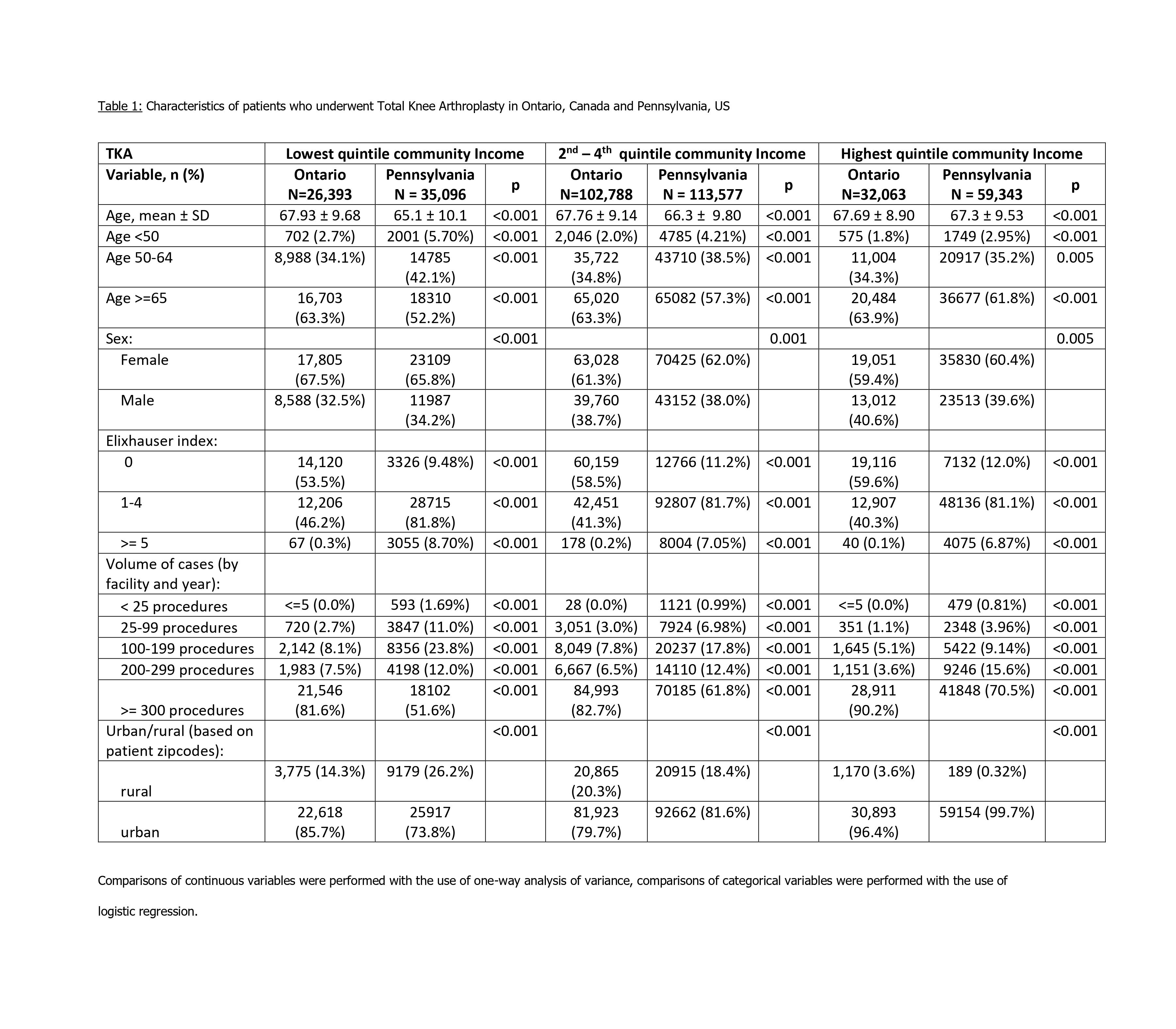

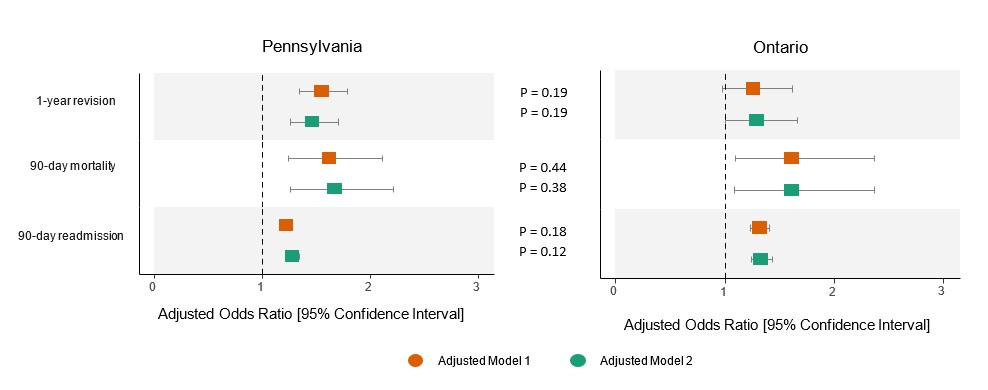 Figure 1 . Adjusted odds ratio of three TKA outcomes (1-year revision, 90-day mortality, 90-day readmission) for patients who lived in the lowest income quintile compared to patients living in the highest income quintile in Pennsylvania and Ontario. Adjusted model 1 adjusted for age, sex, hospital volume of cases, rural/urban Adjusted model 2 adjusted for age, sex, hospital volume of cases, rural/urban, Elixhauser Index Comparison tests for country differences based on model estimates
Figure 1 . Adjusted odds ratio of three TKA outcomes (1-year revision, 90-day mortality, 90-day readmission) for patients who lived in the lowest income quintile compared to patients living in the highest income quintile in Pennsylvania and Ontario. Adjusted model 1 adjusted for age, sex, hospital volume of cases, rural/urban Adjusted model 2 adjusted for age, sex, hospital volume of cases, rural/urban, Elixhauser Index Comparison tests for country differences based on model estimates
To cite this abstract in AMA style:
Mehta B, Ho K, Ling V, Goodman S, Parks M, Ravi B, Banerjee S, Ibrahim S, Cram P. Variations in Total Knee Replacement Utilization and Outcomes in USA and Canada: The Role of Geography and Socioeconomic Factors [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/variations-in-total-knee-replacement-utilization-and-outcomes-in-usa-and-canada-the-role-of-geography-and-socioeconomic-factors/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/variations-in-total-knee-replacement-utilization-and-outcomes-in-usa-and-canada-the-role-of-geography-and-socioeconomic-factors/