Session Information
Session Type: Poster Session A
Session Time: 6:00PM-7:00PM
Background/Purpose: Kawasaki disease (KD) is the leading cause of acquired heart disease in children in North America. Initial treatment with IVIG has significantly reduced the risk of developing coronary artery aneurysms (CAA). However, 10-20% of children with KD fail to respond to the first dose of IVIG (refractory KD) and have an increased risk of developing CAA. The best treatment to prevent CAA in IVIG-refractory KD is currently unknown. The purpose of this survey was to determine treatment preferences of pediatric rheumatologists (PR) in North America to inform future development of consensus treatment plans (CTPs) for children with IVIG-refractory KD.
Methods: The CARRA Refractory KD Workgroup developed a 34-item web-based survey with clinical cases and sent it to 102 randomly selected voting members of CARRA in March 2022. The survey asked participants about their practice settings, when patients should be treated for refractory KD and medication choices for treatment of refractory KD. Respondents who had not treated refractory KD in the previous 3 years were excluded.
Results: The response rate was 82%. A total of 57 pediatric rheumatologists completed the refractory KD questionnaire (Figure 1). There was a wide variation of clinical experience including years in practice and number of refractory KD patients treated. Most of the respondents (86%) were consultants and 9% were members of the primary care team for KD at their institution (Figure 2). While 54% of the 57 respondents considered a temperature 100.4 F (38C) at 36 hours after the completion of the first dose of IVIG warranted treatment for IVIG-refractory KD. Another 33% of questionnaire participants considered refractory KD at 24 hours post IVIG, 11% at 48 hours and 2%- other. The therapeutic choices for IVIG-refractory KD varied among respondents, with important differences based on the presence or absence of CAA. Refractory KD with no CAA: 83% of n=56 respondents would continue treatment with IVIG, of which 63% would give IVIG alone and 20% would give IVIG with corticosteroids (CS). 11% would give only daily IV/PO CS. 5% added Infliximab to their treatment regimen in patients with normal CAs. Refractory KD with non-giant CAA: 73% of n=55 would continue treatment with IVIG, of which 15% would give IVIG alone, 40% would treat with IVIG and CS, and 13% would treat with IVIG, CS and Infliximab. 13 % would treat with Infliximab and CS without additional IVIG. There were 23 different treatment regimens among the respondents, primarily because of varying CS doses/routes. (Figure 3) Refractory KD with giant CAA: 69% of n=55 would continue treating with IVIG, of which 5% would treat with IVIG alone, 24% with IVIG and CS, and 20% would treat with IVIG, CS and Infliximab. 20% would treat with Infliximab and CS, but not IVIG. There were 32 different treatment regimens among the respondents, primarily because of varying CS doses/routes.
Conclusion: Treatment of IVIG-refractory KD varies widely among North American pediatric rheumatologists, particularly in the presence of CAA. The results of this survey support the need to conduct comparative effectiveness research to identify the most effective therapy for the prevention of CAA and to improve outcomes in children with IVIG-refractory KD.
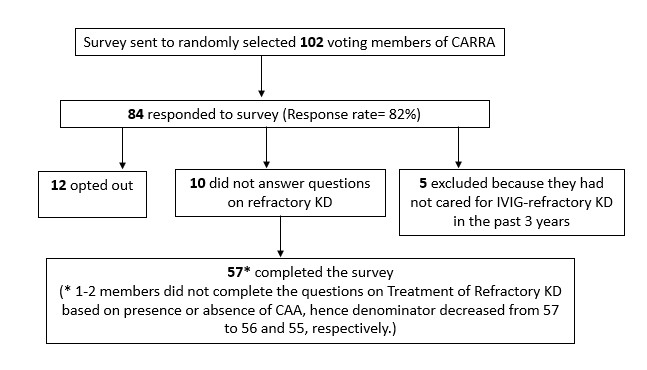 Figure 1. Survey Response and Completion in Numbers
Figure 1. Survey Response and Completion in Numbers
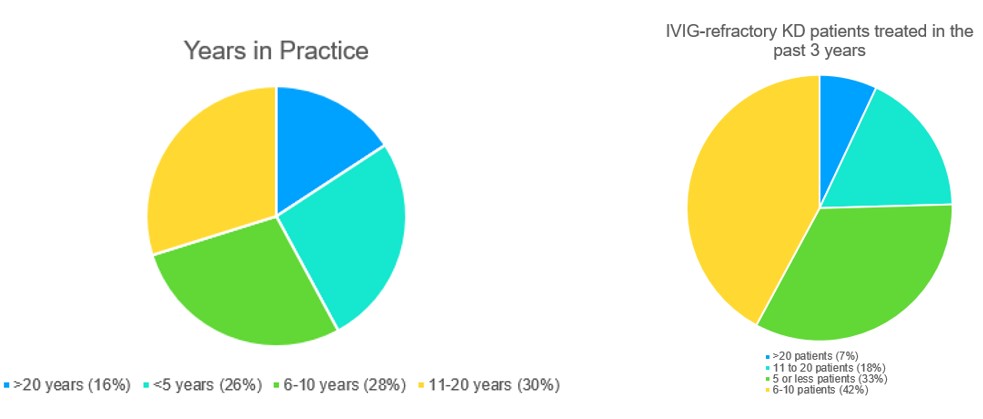 Figure 2. Experience of Survey Respondent Pediatric Rheumatologists
Figure 2. Experience of Survey Respondent Pediatric Rheumatologists
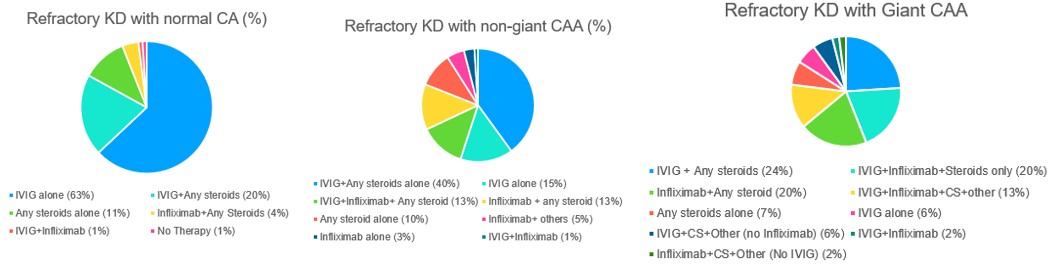 Figure 3. Variability in Treatment of IVIG-refractory KD with and without CAA among Pediatric Rheumatologists
Figure 3. Variability in Treatment of IVIG-refractory KD with and without CAA among Pediatric Rheumatologists
To cite this abstract in AMA style:
Ibanez D, Lang B, Yalcindag A, Wagner-Weiner L, Shalen J, Schikler K, Akoghlanian S, Bukulmez H, Hayward K, Lapidus S, Ramirez A, Sundel R, Yildirim-Toruner C, Investigators C. Variation in Treatment Approaches to IVIG- Refractory Kawasaki Disease (KD) Among Pediatric Rheumatologists: The Childhood Arthritis and Rheumatology Research Alliance (CARRA) Treatment of Refractory KD Survey [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 4). https://acrabstracts.org/abstract/variation-in-treatment-approaches-to-ivig-refractory-kawasaki-disease-kd-among-pediatric-rheumatologists-the-childhood-arthritis-and-rheumatology-research-alliance-carra-treatment-of-refractory/. Accessed .« Back to 2023 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/variation-in-treatment-approaches-to-ivig-refractory-kawasaki-disease-kd-among-pediatric-rheumatologists-the-childhood-arthritis-and-rheumatology-research-alliance-carra-treatment-of-refractory/