Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: ANCA-associated vasculitis (AAV) causes sinus symptoms that impact quality of life. The 22-item Sinonasal Outcome Test (SNOT-22) is a patient-reported outcome measure to assess symptoms and quality of life in chronic rhinosinusitis but has not been well-studied in AAV. We compared SNOT-22 scores during remission and active disease in AAV patients with and without sinus involvement and investigated if SNOT-22 scores can predict subsequent relapse.
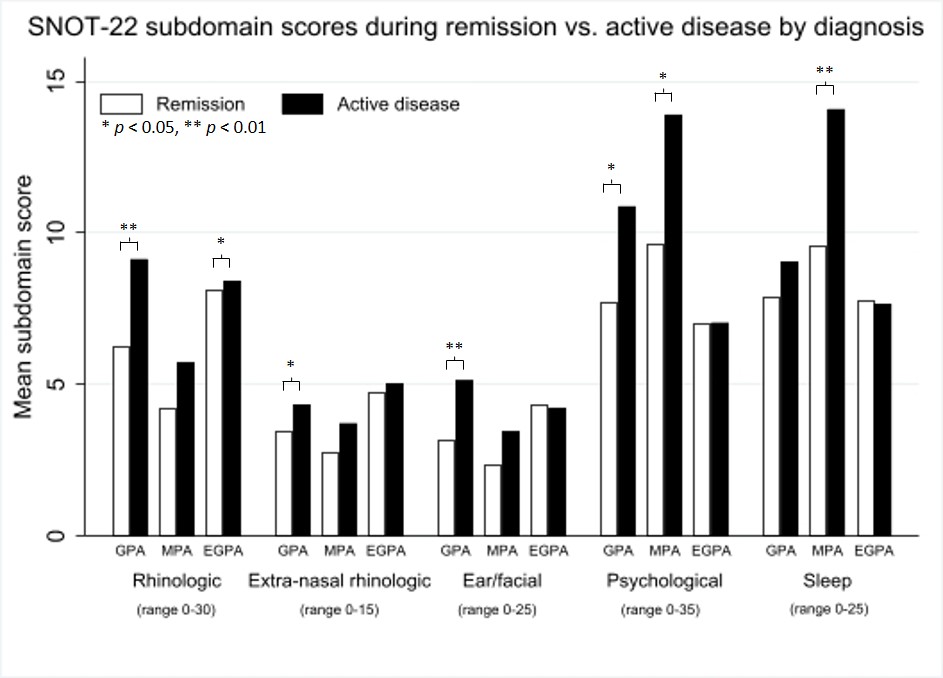
Methods: Subjects with AAV (granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), eosinophilic granulomatosis with polyangiitis (EGPA) based on 1990 ACR classification criteria or Chapel Hill Consensus Conference nomenclature) and healthy controls were followed longitudinally with measures of disease activity [BVAS/WG, physician global assessment (PGA)], SNOT-22, and treatment. SNOT-22 questions are scored on a 0-5 scale with higher scores for worse symptoms and include 5 subdomains (rhinologic, extra-nasal rhinologic, ear/facial, psychological, sleep). Generalized estimating equations evaluated the association between SNOT-22 scores and disease activity. Models were adjusted for concomitant seasonal allergies and use of antibiotics, immunosuppressive drugs, and sinus rinses.
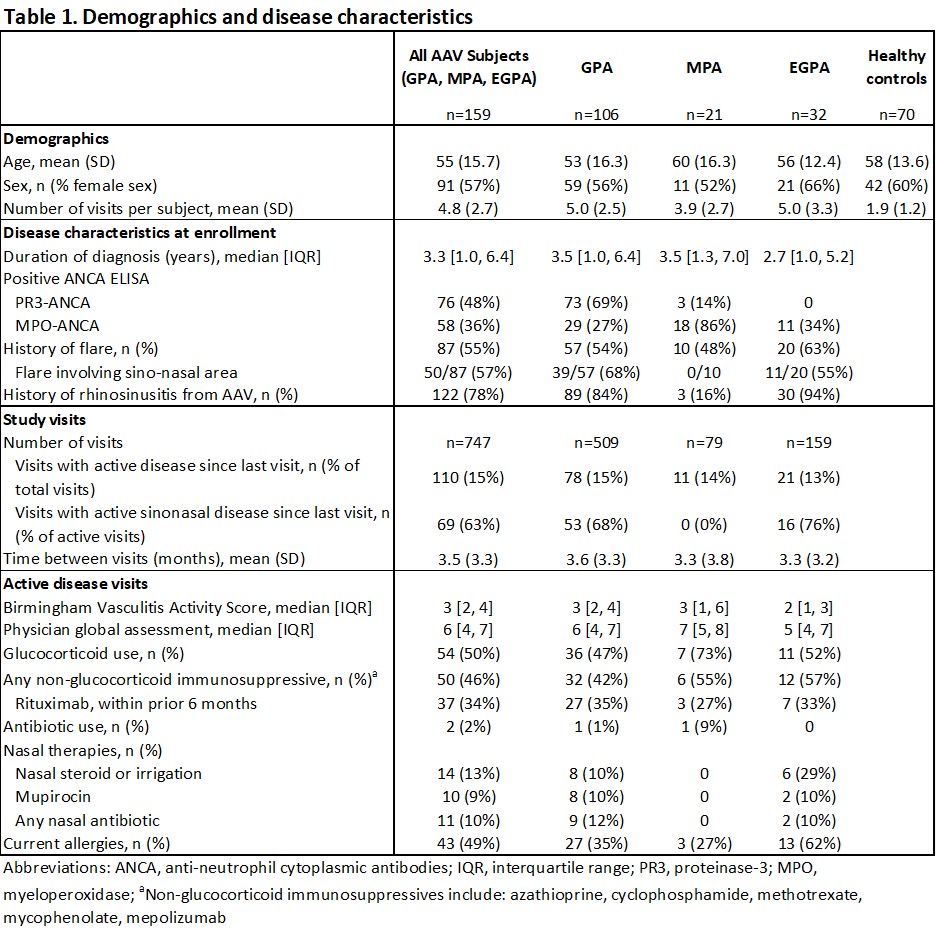
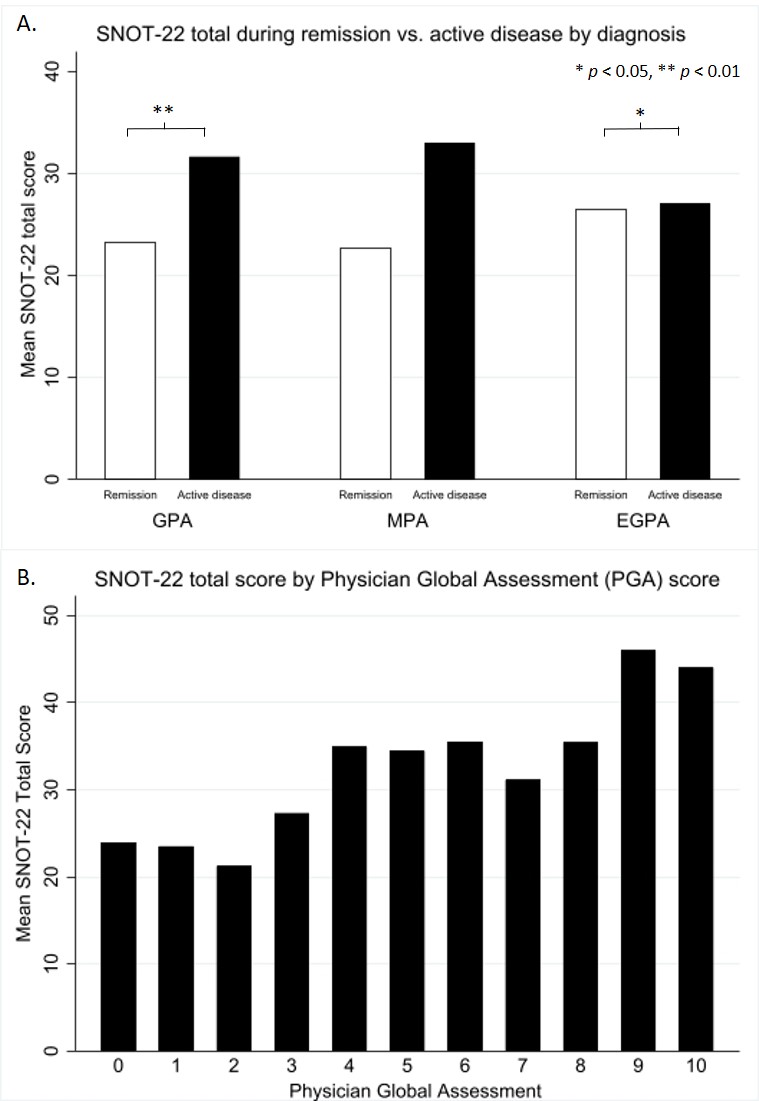
Results: 159 AAV subjects (106 GPA, 21 MPA, 32 EGPA) with 747 visits (110 active disease visits, mean interval 3.5 months) and 70 controls were included (Table 1). Baseline SNOT-22 total scores were higher in AAV vs. controls (mean (SD): 27.5 (1.6) vs. 15.4 (2.1), p< 0.01) and higher for AAV subjects with vs. without sinus involvement (mean (SD): 30.3 (20.5) vs. 17.8 (13.2), p< 0.01). Adjusted SNOT-22 total scores were significantly higher during active disease vs. remission for GPA and EGPA but not MPA (Figure 1A). Subgroup analyses demonstrated similar results among subjects with a history of sinonasal involvement but not among subjects without baseline sinonasal disease (p=0.3). For all AAV, higher PGA was associated with higher SNOT-22 total (Figure 1B). In GPA, active disease was associated with higher scores in each SNOT-22 subdomain except sleep. Compared to remission visits, active disease was associated with worse scores occurred in the psychological and sleep subdomains for MPA and in the rhinologic subdomain for EGPA (Figure 2). Prior SNOT-22 total scores were not associated with subsequent relapse among all visits, but when limiting visits to those 2 months apart, increase in SNOT-22 score at prior visits was associated with subsequent relapse (adj OR 1.15 per score change of 5, 95% CI: 1.0-1.3, p=0.03).
Conclusion: In AAV, SNOT-22 scores are higher during active disease vs. remission particularly among patients with previous sinus involvement. The subdomains impacted most by disease activity differ by disease type. When measured within 2 months, change in SNOT-22 scores at remission are associated with subsequent relapse. SNOT-22 may be an informative patient-reported outcome measure to monitor disease activity in AAV patients.
To cite this abstract in AMA style:
Romich E, Chou S, Rhee R. Utility of the 22-Item Sinonasal Outcome Test Patient-Reported Outcome Instrument in ANCA-Associated Vasculitis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/utility-of-the-22-item-sinonasal-outcome-test-patient-reported-outcome-instrument-in-anca-associated-vasculitis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/utility-of-the-22-item-sinonasal-outcome-test-patient-reported-outcome-instrument-in-anca-associated-vasculitis/