Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: The identification of immune checkpoint inhibitor (ICI)-induced inflammatory arthritis (ICI-IA) using administrative data would provide a valuable advance in the investigation of ICI-IA. The utilization of ICD coding for identifying these patients has yet to be evaluated. This investigation reports the ICD codes assigned to ICI-IA patients in the Veterans Health Administration (VHA) Rheumatology clinics to determine if these codes are sufficiently specific to accurately identify ICI-IA patients.
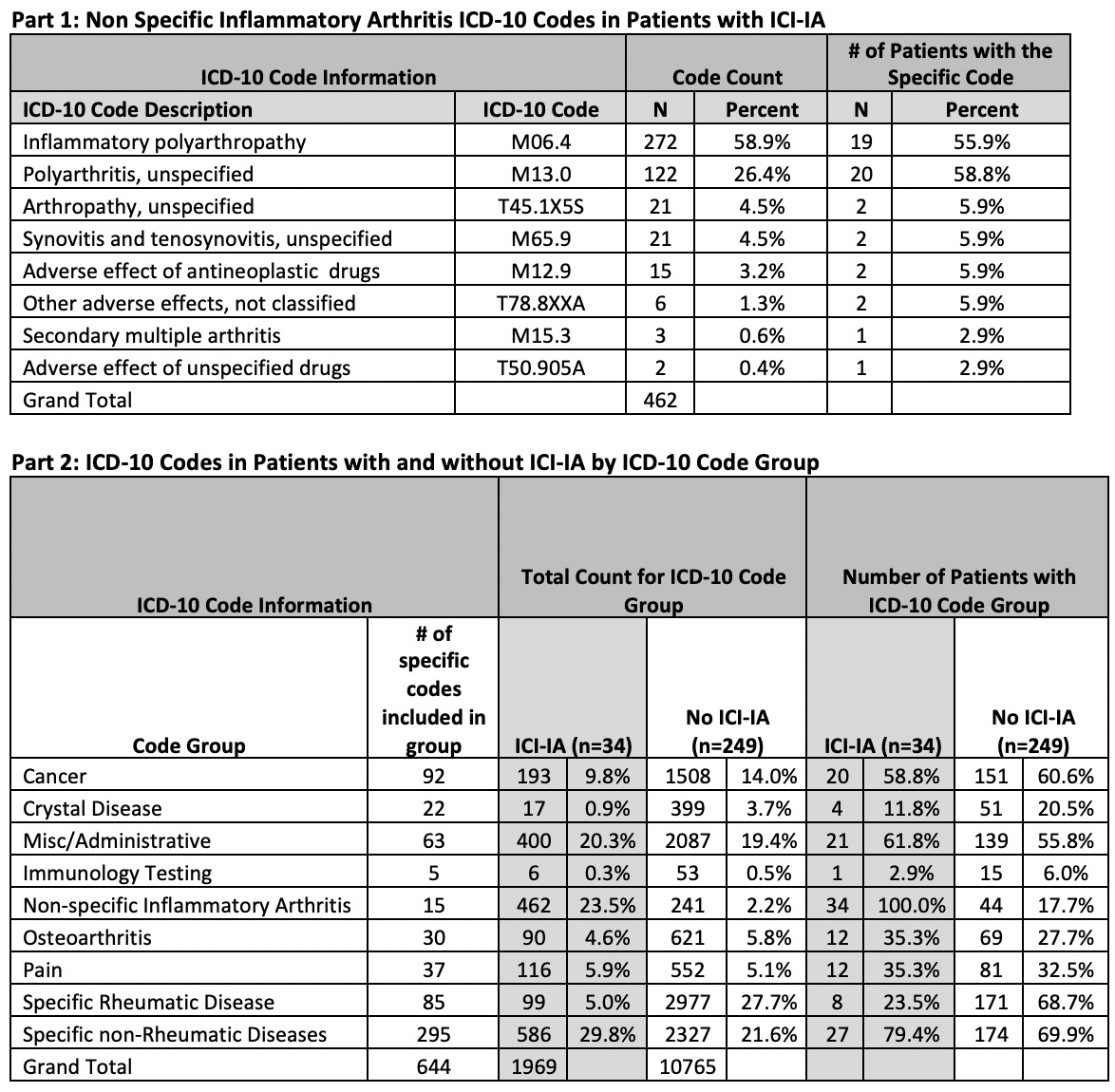
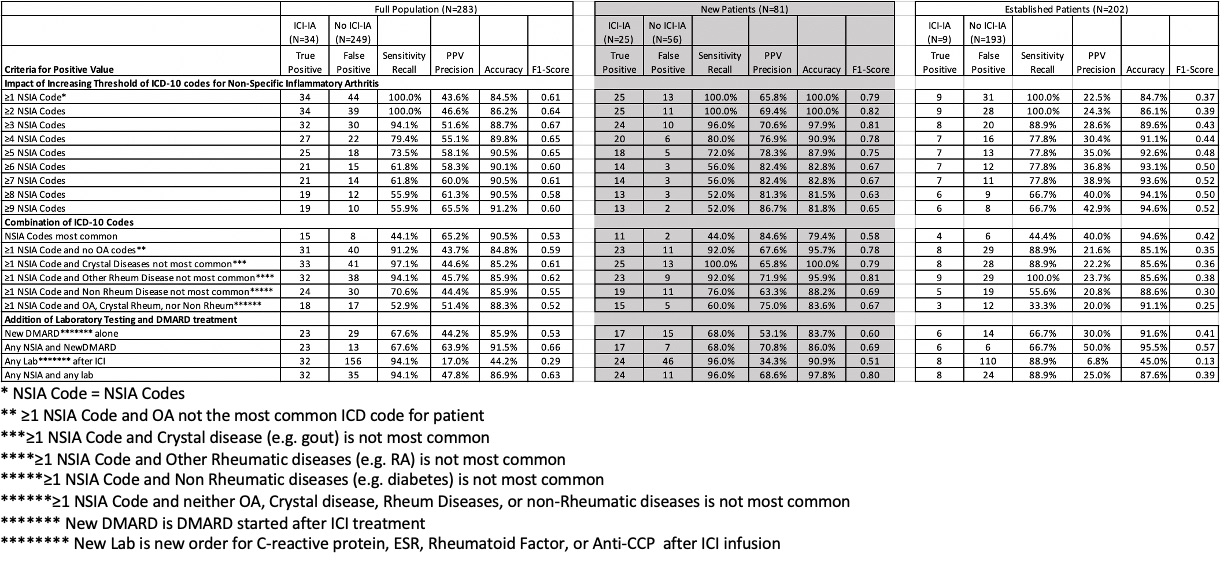
Methods: The Corporate Data Warehouse (CDW) identified ICI treated Veterans with one or more VHA Rheumatology clinic visit(s) within 6 months from ICI initiation between 2011 and 2024. A structured electronic medical record (EMR) review using Microsoft Access identified ICI-IA patients and ICD-10 codes for each rheumatology clinic visit. ICD codes were classified into groups (Table 1). Codes recorded in ICI-IA patients for non-specific inflammatory arthritis (NSIA) were specifically noted. To determine the discrimination ability of these codes for classifying patients with ICI-IA and patients without ICI-IA, we compared overall ICD codes and specifically the number of NSIA ICD codes for patients with and without ICI-IA in both new and established patients. We then evaluated the potential benefit excluding other non-NSIA ICD classification groups, and adding on laboratory and pharmacy data to the ICD-10 codes.
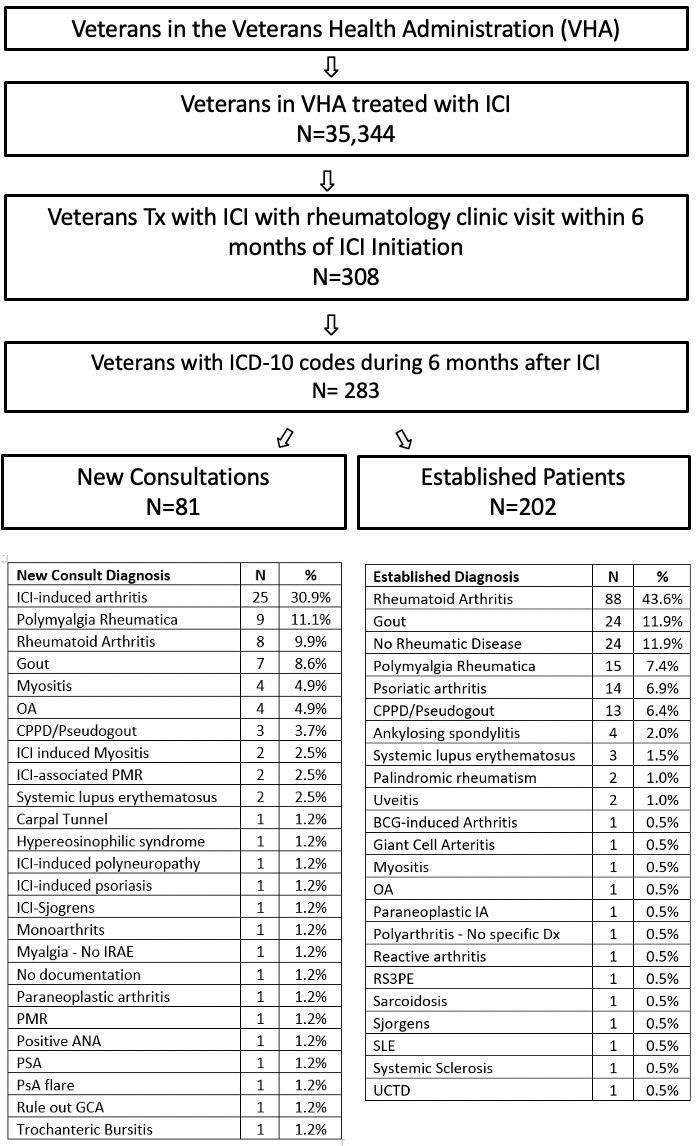
Results: In the 35,344 Veterans receiving an ICI there were 308 with VHA Rheumatology Clinic visit within 6 months of ICI initiation, 283 were included in final analysis (Figure 1). There were 81 new patients and 202 established patients. ICI-IA (30.9%) and Rheumatoid arthritis (43.6%) were the most common diagnoses in new and established patients respectively. The most common NSIA code in patients with ICI-IA was inflammatory polyarthropathy (58.9%) (Table 1). Of the 34 patients with known ICI-IA, all had ≥ 1 NSIA codes with 19 (55.9%) having an inflammatory polyarthropathy code and 20 (58.8%) a polyarthritis code. NSIA codes were used in 44 (17.7%) of patients without ICI-IA. The ability of an NSIA ICD code to identify those with ICI-IA in new patients demonstrated that the PPV ranged from 65.8%-86.7%, accuracy from 81.8%-100%, and F1 score from 0.65 to 0.82, pending the number of NSIA codes (Table 2). For established patients the PPV was 22.5%- 42.9%, accuracy was 84.7%- 94.6% and F1 score of 0.37- 0.52. Increasing the required number of NSIA codes improved identification of ICI-IA in all categories of patients. The exclusion of non-NSIA code groups and addition of laboratory and pharmacy data did not result in significant improvement in the identification of ICI-IA.
Conclusion: This study demonstrates that the current coding system effectively identifies patients with ICI-IA among new patients but is limited by the lack of specificity of ICD-10 codes for the differentiation of ICI-IA from other rheumatic diseases in established patients. Inflammatory polyarthropathy and polyarthritis were the most frequently used NSIA codes. This study demonstrates the value and limitations of using ICD-10 codes to identify ICI-IA patients in a large database.
To cite this abstract in AMA style:
Braaten T, O’Sullivan M, Patel s, brian S, Rojas J, Cannon g, Lai m. Use of ICD Codes for the Identification of Patients with Immune Checkpoint Inhibitor Induced Inflammatory Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/use-of-icd-codes-for-the-identification-of-patients-with-immune-checkpoint-inhibitor-induced-inflammatory-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/use-of-icd-codes-for-the-identification-of-patients-with-immune-checkpoint-inhibitor-induced-inflammatory-arthritis/