Session Information
Date: Tuesday, November 7, 2017
Title: Osteoarthritis – Clinical Aspects Poster II: Observational and Epidemiological Studies
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Excessive cartilage degradation is a known characteristic of osteoarthritis (OA), and several methods of quantification of cartilage degradation exist. Biomarkers such as urinary C-telopeptide fragments resulting from inflammatory destruction of collagen type II (uCTX-II) have been shown to be associated with disease severity and pain in OA, yet the tissue-origin of uCTX-II has been disputed.
The purpose of this analysis was to investigate the potential association between OA in single and multiple joints at different radiographic stages on circulating levels of uCTX-II and biomarkers of bone resorption and bone formation; serum and urine C-telopeptide of collagen type I, CTX-I, and serum osteocalcin, respectively.
Methods: Pooled, pre-treatment baseline data of two phase III randomized clinical trials (NCT00486434 and NCT00704847) in patients with radiographic OA of at least one knee joint were analyzed post-hoc. Key inclusion criteria were knee OA with a Kellgren and Lawrence (KL) score of 2 or 3, and pain of at least 150 mm out of 500 mm using the WOMAC pain subscore, of at least one knee. A subgroup with available urine samples (N=1200) was analyzed for this report. Baseline levels of serum and urine CTX-I, urine CTX-II and serum osteocalcin were analysed using validated enzyme-linked immunosorbent assays and analyzed for associations with combined KL-scores for both knees, and cumulative KL-scores to assess the individual biomarker contribution of joints at different disease stages using multiple pairwise comparisons. KL score of 0 was defined as absence of OA, while all knees with KL scores of ≥ 1 were defined as OA joints.
Results: Unilateral knee OA was present in 4.1 % of patients in the study. 63.1 % of patients had bilateral, early OA, 10.1 % had bilateral late OA, and 22.0 % had bilateral OA of mixed stages. No patients had unilateral OA with late stage disease. Patients with bilateral, late-stage OA had significantly higher levels of uCTX-II compared to patients with earlier OA. The presence of at least one KL-4 joint appeared to markedly increase the level of CTX-II regardless of the KL-score of the contralateral knee joint. Levels of CTX-I and osteocalcin were not significantly different between KL-grades.
Figure 1
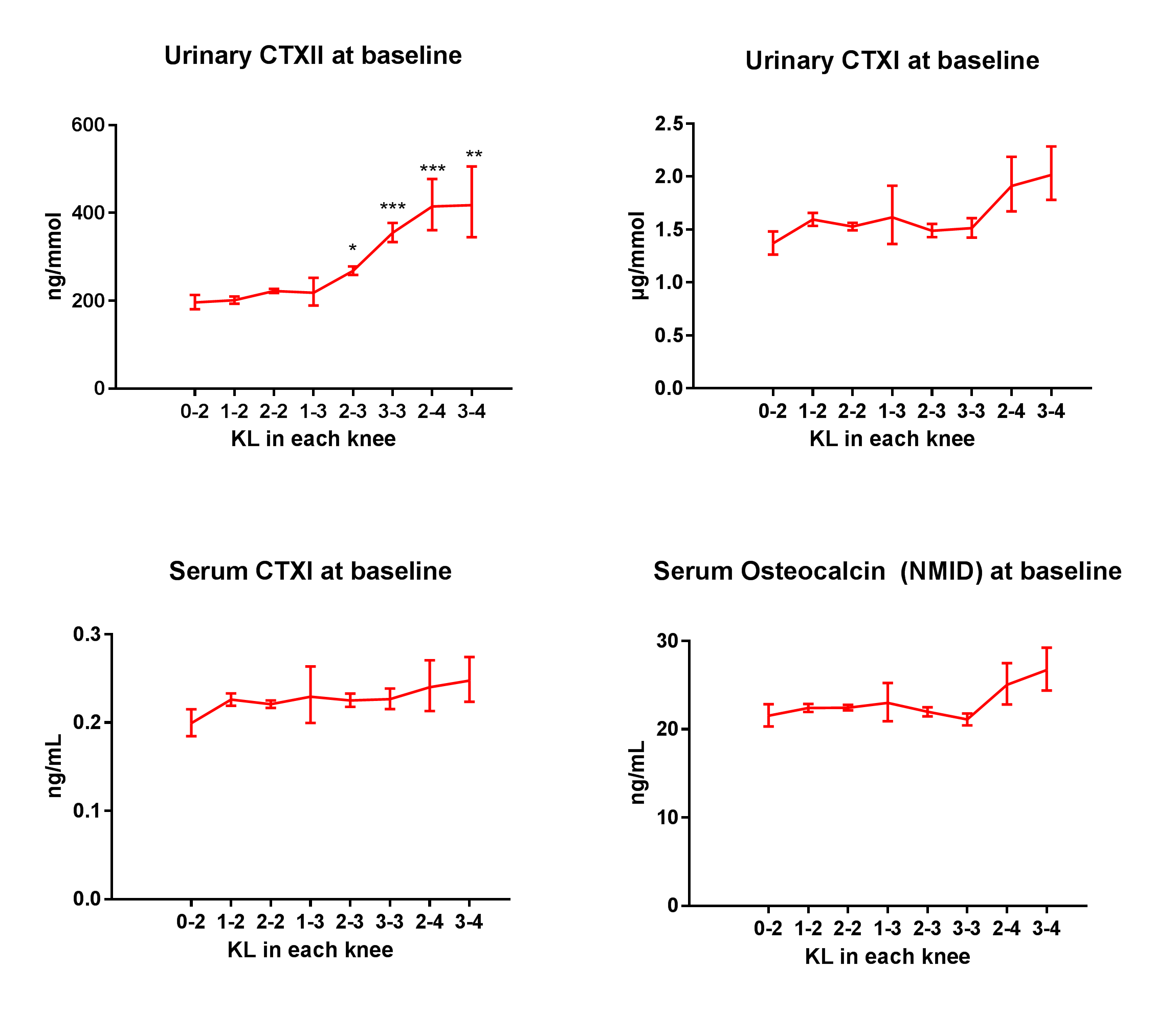
Association between geometric mean concentration of uCTX-II, sCTX-I and osteocalcin and Kellgren-Lawrence radiographic stage in the knees of 1200 OA patients. Asterisks indicate statistically significant (p<0.05) difference to the group of subjects with the lowest cumulative KL-score, i.e. a KL-grade of 0 in one knee and 2 in the other (“0-2”).
To cite this abstract in AMA style:
Bihlet AR, Byrjalsen I, Bay-Jensen AC, Andersen J, Christiansen C, Riis BJ, Karsdal MA. Urine CTX-II, CTX-I, Osteocalcin, and Radiographic Severity of Multiple OA Knee Joints: Does CTX-II Originate from Bone or Cartilage? [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/urine-ctx-ii-ctx-i-osteocalcin-and-radiographic-severity-of-multiple-oa-knee-joints-does-ctx-ii-originate-from-bone-or-cartilage/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/urine-ctx-ii-ctx-i-osteocalcin-and-radiographic-severity-of-multiple-oa-knee-joints-does-ctx-ii-originate-from-bone-or-cartilage/