Session Information
Date: Saturday, November 6, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster I: Cardiovascular Pulmonary Disease (0268–0295)
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Interstitial lung disease (ILD) frequently complicates the rheumatoid arthritis (RA) disease course, leading to significant morbidity and premature mortality. RA-ILD may be underdiagnosed or detected later in the disease course because of inadequate screening methods. Several peripheral blood biomarkers have been investigated in RA-ILD, but the performance of composite biomarker profiles for identifying RA-ILD in larger RA cohorts is unknown.
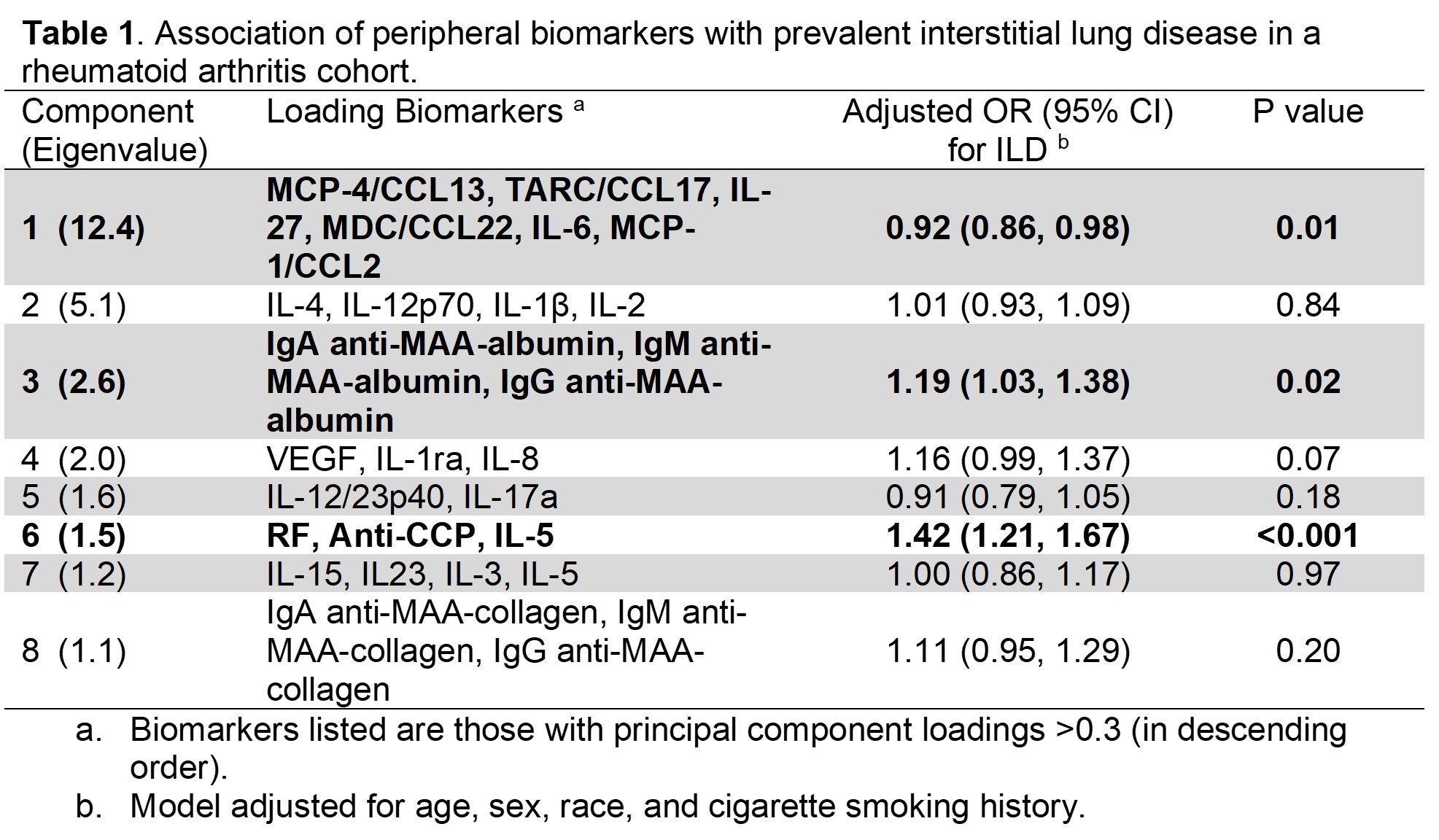
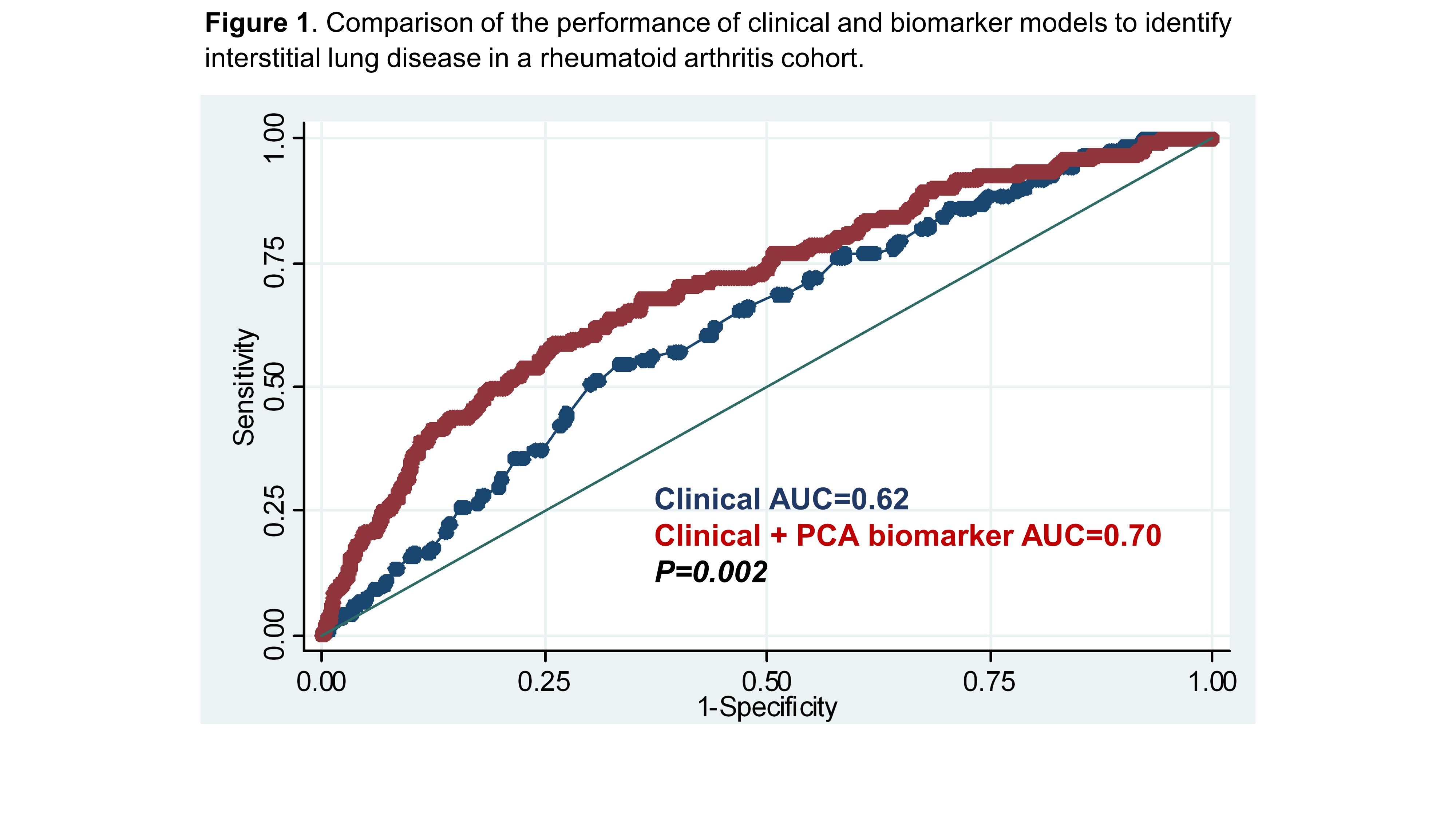
Methods: We studied participants in a prospective cohort of U.S. Veterans with RA fulfilling ACR criteria. Demographics, RA history, smoking status, and ACR core measures are collected regularly, complementing a biorepository of peripheral blood samples obtained at enrollment. We measured 33 cytokines and chemokines (via the MesoScale platform), RF concentration (by nephelometry), anti-CCP concentration (by 2nd generation ELISA), and anti-malondialdehyde acetaldehyde (MAA) antibody concentration (IgA, IgM, and IgG anti-MAA-albumin and anti-MAA-collagen, all by ELISA) from banked serum. Prevalent ILD was determined through validated methods that included detailed, systematic review of medical records for clinical diagnoses, imaging findings, and biopsy reports. The aforementioned biomarkers were log-transformed and standardized. Subsequently, principal component analysis (PCA) was performed, retaining components with eigenvalues >1. The ability of the resultant principal component (PC) scores to improve ILD identification was assessed in multivariable logistic regression models. Receiver operating characteristic curves were generated for clinical (age, sex, race, and cigarette smoking history) and clinical + PC score models.
Results: Among 2,044 RA patients (86% male, mean age 64 years, 79% smoking history), 121 had prevalent ILD. PCA of 33 cytokines/chemokines and 8 RA autoantibodies identified 8 unique biomarker PCs. Biomarkers loading onto each PC after orthogonal rotation are shown in Table 1. Kaiser-Meyer-Olkin (KMO) testing showed high adequacy for PCA (KMO=0.93). PC 1 scores (characterized by inflammatory monocyte/macrophage mediators) were negatively associated with the presence of ILD while PC 3 scores (anti-MAA-albumin) and PC 6 scores (RF & anti-CCP) were positively associated with the presence of ILD (Table 1). Adding PC scores to a clinical only model improved the discrimination of ILD in the RA cohort, evidenced by an increase in the area under the curve (AUC) from 0.62 to 0.70 (p=0.002; Figure 1).
Conclusion: In a large RA cohort with validated ILD diagnoses, we found that unsupervised machine learning of 33 cytokines and chemokines and 8 autoantibodies improved the identification of RA-ILD. RA-related autoantibodies (anti-MAA-albumin, RF, and anti-CCP) were the peripheral biomarkers most closely associated with the presence of RA-ILD, suggesting that serologic antibody responses may have the greatest potential for identifying ILD or at-risk patients. Cohort-wide screening for RA-ILD using peripheral blood biomarkers shows promise as an ILD screening modality and should be further validated in other cohorts.
To cite this abstract in AMA style:
England B, Ascherman D, Duryee M, Hunter C, Yang Y, Roul P, Sayles H, Yu F, Poole J, Baker J, Thiele G, Mikuls T. Unsupervised Machine Learning of Expanded Autoantibodies, Cytokines, and Chemokines Improves the Identification of Interstitial Lung Disease in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/unsupervised-machine-learning-of-expanded-autoantibodies-cytokines-and-chemokines-improves-the-identification-of-interstitial-lung-disease-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/unsupervised-machine-learning-of-expanded-autoantibodies-cytokines-and-chemokines-improves-the-identification-of-interstitial-lung-disease-in-rheumatoid-arthritis/