Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Identifying novel biomarkers of disease activity could improve outcomes by facilitating personalized approaches to treatment decisions in ANCA-associated vasculitis. Biomarkers of disease activity used in day-to-day practice include PR3- or MPO-ANCA, CRP, and ESR, but these are unreliable. Few studies have examined a limited number of circulating proteins as biomarkers, identifying some candidates (e.g., BCA-1, MMP-3, TIMP-1). We previously leveraged a high-throughput, unbiased approach to investigate 92 potential biomarkers in AAV patients and identified 5 potential biomarkers: MCP3, TNFSF-14, OSM, Flt3L, and SCF. The objective of this study was to further investigate the association of 5 novel protein biomarkers with AAV disease activity.
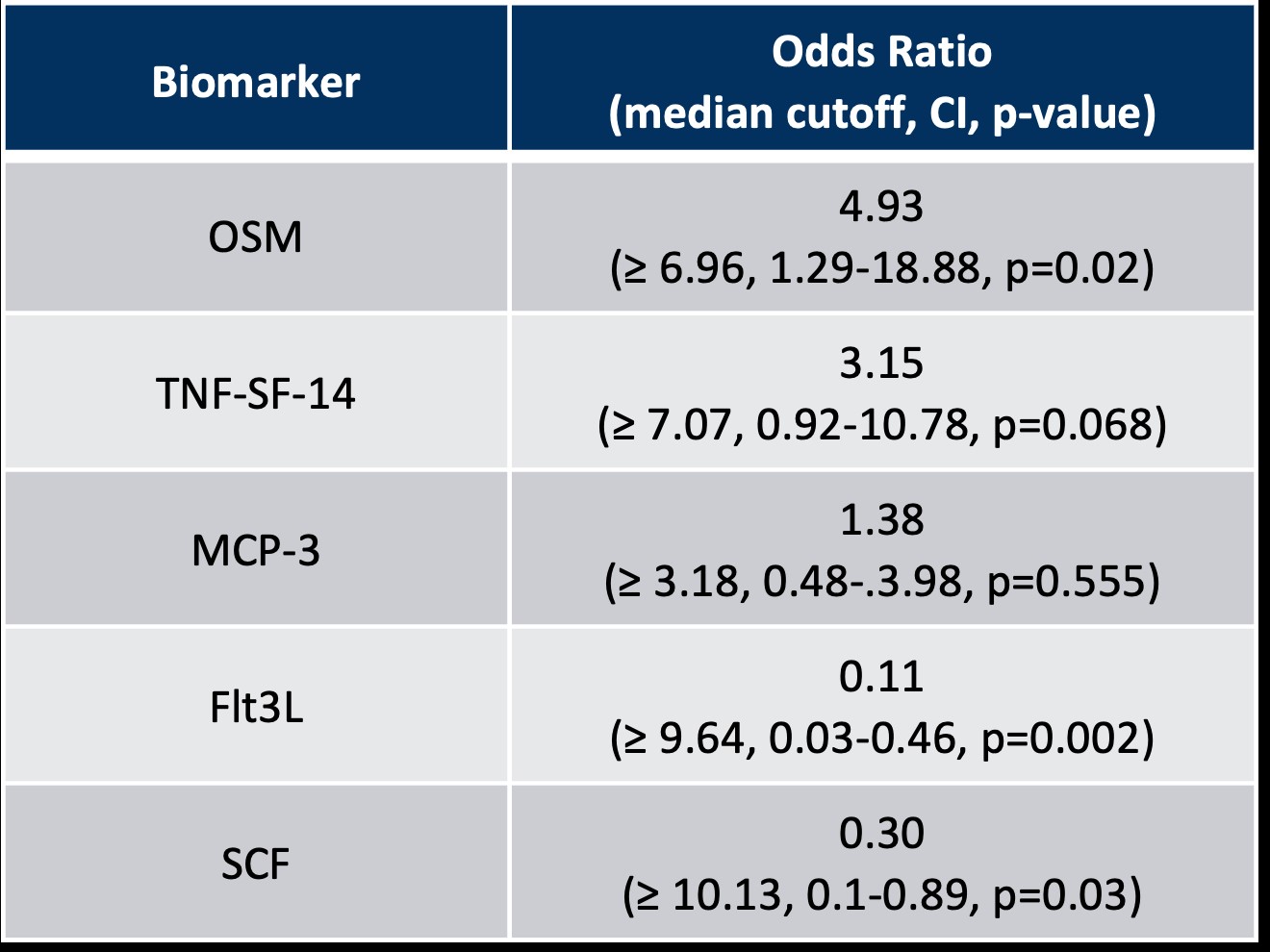
Methods: Serum samples from n=78 patients with AAV were retrieved from a large biobank. We classified disease activity as “Active” or “Remission” at sample collection. The Olink high-throughput proteomic assay was used to measure circulating protein levels. Measurements of ESR, CRP, white blood cell (WBC) count and platelets collected for clinical purposes were extracted from the electronic medical record. We compared the levels of these potential biomarkers in active disease vs remission. Using the median value of each biomarker in the cohort as cut-off values, we determined the odds ratio (OR), the area under the receiver operating curve (AUC) of the association of abnormal biomarker with active disease, and a multivariate logistic regression to adjust for steroid use, sex, age and ANCA type.
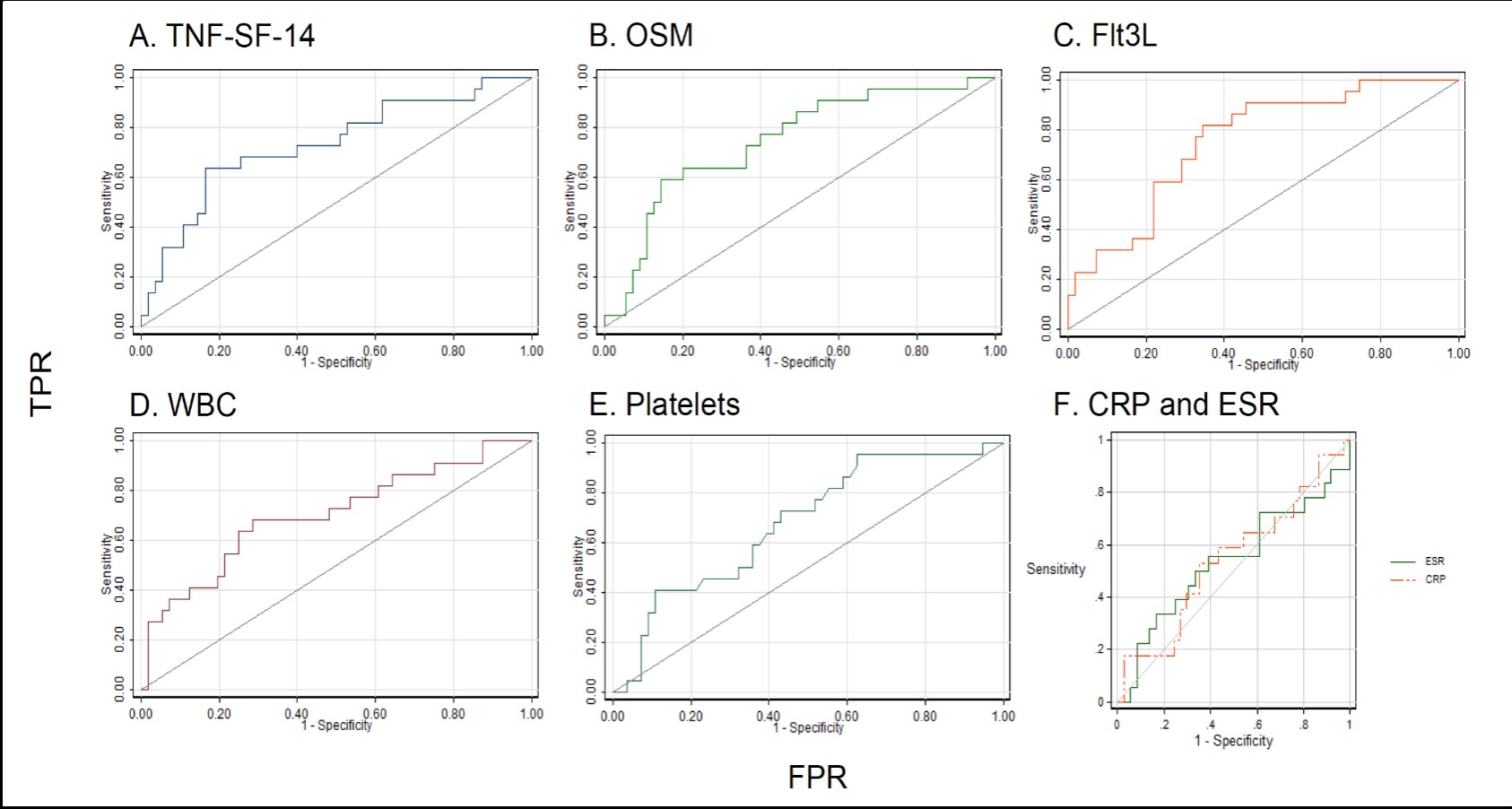
Results: The mean age was 57.3 +/- 17.6, 55% were female, and 28% had active disease at sample collection. When comparing active disease vs remission, abnormal levels of OSM, TNF-SF-14, Flt3L, and SCF differentiated disease states: OR of 5.10 (p=0.005), 3.71 (p=0.017), 0.13 (p=0.001), and 0.34 (p=0.04), respectively. AUC analysis indicated that TNF-SF-14 (0.73, CI 0.60-0.86), OSM (0.75, CI 0.62-0.87), and Flt3L (0.76, CI 0.64-0.87) were more strongly associated with active disease than other biomarkers, including WBC (0.70, CI 0.57-0.84), platelets (0.68, CI 0.55-0.81), CRP (0.55, CI 0.38-0.72), and ESR (0.55, CI 0.37-0.72).After adjusting for steroid use, sex, age, and ANCA type, we found that only OSM and Flt3L differentiated active disease from remission.
Conclusion: Using a high-throughput, unbiased proteomics approach, we further investigated novel candidate markers differentiating active AAV disease from remission. These proteins likely reflect different states of immune activation during active disease and outperform conventional inflammatory markers (e.g., CRP, ESR) as well as WBC and platelets. Our study has certain limitations including sample size, a cross-sectional study design, and requires validation across diverse, longitudinal cohorts. The potential for biomarkers that accurately identify those individuals in remission compared to active disease may facilitate tailored, personalized therapeutic intervention, which avoids unnecessary exposure to the toxic side effects of immunomodulatory agents.

To cite this abstract in AMA style:
Atallah N, Panossian V, Fu X, Cook C, Wallace Z. Unbiased Proteomic Approach to Identify Novel Biomarkers of Disease Activity in ANCA- Associated Vasculitis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/unbiased-proteomic-approach-to-identify-novel-biomarkers-of-disease-activity-in-anca-associated-vasculitis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/unbiased-proteomic-approach-to-identify-novel-biomarkers-of-disease-activity-in-anca-associated-vasculitis/