Session Information
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: With increased use of musculoskeletal ultrasound (US) among rheumatologists, it will be necessary to understand what additional clinical information may be derived from US joint assessment versus routine clinical assessment in patients with rheumatoid arthritis (RA). Our study aims to gain further insight into this by studying the severity of joint damage in RA patients classified based on their US joint inflammation findings and their disease activity score at 28 joints (DAS28). By comparing with DAS28, this cross-sectional study mimics what happens in routine clinical practice, whereby clinicians often rely on routine clinical measures (like DAS28) for RA disease activity assessment.
Methods: US power Doppler (PD) and grey scale (GS) joint inflammation were graded semi-quantitatively (0-3), while bone erosion was scored dichotomously (Yes=1 or No=0) at each joint recess. Patients were categorized into 4 US patient groups: group 1 (PD positive and GS ≥median score of 35.5); group 2 (PD negative and GS ≥ median score); group 3 (PD positive and GS < median score); group 4 (PD negative and GS < median score). US erosion scores were compared (a) between patients in groups 1 vs. 4, groups 2 vs. 4 and groups 3 vs. 4 and (b) between patients with high ( > 5.1), moderate (≥ 3.2 and ≤ 5.1) and low (≥ 2.6 and < 3.2) DAS28 scores versus those in DAS28 remission (< 2.6). All comparative analyses were performed using the unpaired student’s T-test.
Results: 1080 joints and 1800 joint recesses from bilateral elbows, wrists, ankles and small joints of the hands and feet were scanned in 30 adult RA patients with the following baseline characteristics: 76.7 % Chinese; 93.3% female; mean (SD) DAS28 of 3.58 (1.20); mean (SD) disease duration of 70.3 (61.2) months; 90% on conventional DMARD (methotrexate, sulfasalazine, hydroxychloroquine and/or leflunomide). Table 1 summarizes the comparison of US erosion scores between the 4 ultrasound patient groups. The mean (95% CI) US erosion scores were significantly higher (p=0.026) for groups 1 vs. 4 (9.75 (6.69, 12.81) vs. 3.4 (1.11, 5.69), respectively) with a difference (95% CI) of 6.35 (0.78, 11.83). US erosion scores were, however, not significantly different (P-values all >0.05) for patients in groups 2 vs. 4 and 3 vs. 4. Table 2 summarizes the comparison of US erosion scores between the DAS28 disease severity categories. The US erosion scores of patients with high, moderate and low DAS28 disease severity categories were not significantly different (P-values all >0.05) from that of patients in DAS28 remission.
Conclusion: US joint inflammation assessment – and not DAS28 – is reflective of the severity of joint damage in RA patients. Specifically, the severity of US-detected bone erosions was significantly greater when both positive PD and a greater degree of GS joint inflammation were present. This association was not observed when either component was absent. Given this advantage of US joint inflammation assessment over DAS28 assessment, the former may potentially help identify RA patients with a more aggressive disease course requiring more intensive treatment, although this will need to be further evaluated in future studies.
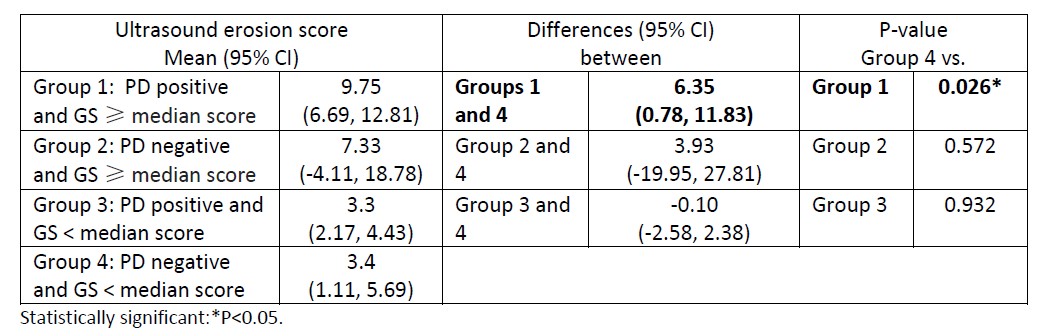 Table 1. Comparison of ultrasound erosion scores between the ultrasound patient groups.
Table 1. Comparison of ultrasound erosion scores between the ultrasound patient groups.
 Table 2. Comparison of ultrasound erosion scores between the DAS28 disease severity categories.
Table 2. Comparison of ultrasound erosion scores between the DAS28 disease severity categories.
To cite this abstract in AMA style:
Tan Y, Li H, Allen Jr J, Thumboo J. Ultrasound Joint Inflammation but Not Disease Activity Score at 28 Joints Is Reflective of the Severity of Joint Damage in Patients with Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/ultrasound-joint-inflammation-but-not-disease-activity-score-at-28-joints-is-reflective-of-the-severity-of-joint-damage-in-patients-with-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ultrasound-joint-inflammation-but-not-disease-activity-score-at-28-joints-is-reflective-of-the-severity-of-joint-damage-in-patients-with-rheumatoid-arthritis/