Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Management of cardiac sarcoidosis remains controversial. Our study aimed to describe our experience using tumor necrosis factor-α-inhibitors (aTNF) in cardiac sarcoidosis treatment.
Methods: This is a retrospective analysis of patients with cardiac sarcoidosis from Northwell Health Rheumatology. Demographics, clinical characteristics, positron emission tomography (PET) and ejection fraction (EF) from either PET or echocardiogram (ECHO) were collected. Patients were grouped as non aTNF, early aTNF start (<2 years of diagnosis), and late aTNF start (>2 years after diagnosis). Two patients, one early aTNF and one late aTNF, had a pre-aTNF EF, but no EF available post aTNF use. They were reassigned to non aTNF group for paired EF analysis, but for baseline and survival analysis, they remained in the original groups. Composite severity PET score (utilizing perfusion, FDG uptake, number of cardiac segments and right ventricular (RV) involvement) was calculated (0-3 – mild; 3-7 – moderate; 5-11- severe). Change in PET severity score or > 10% absolute EF from baseline defined improved, worsened or stable response. Annualized EF change was computed. Descriptive statistics, the Kruskal Wallis, Fisher’s exact, and ANOVA Friedman tests were used to compare groups for continuous and categorical variables.
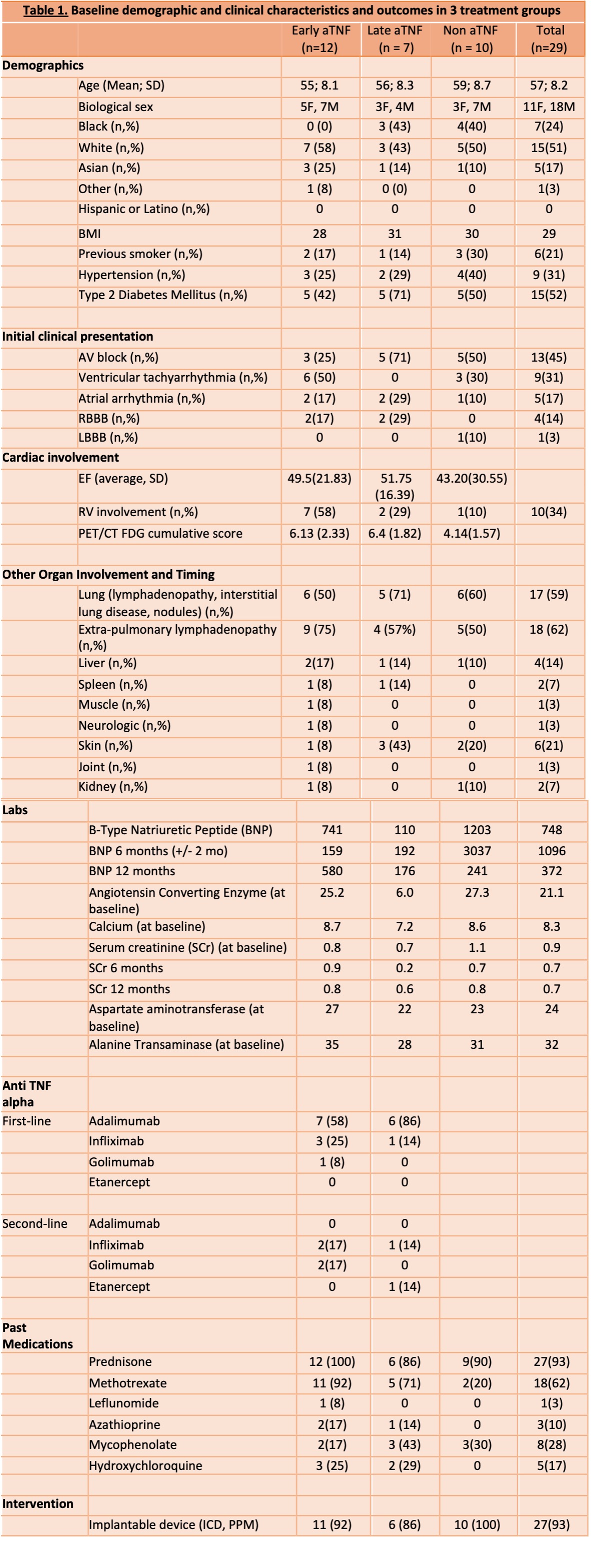
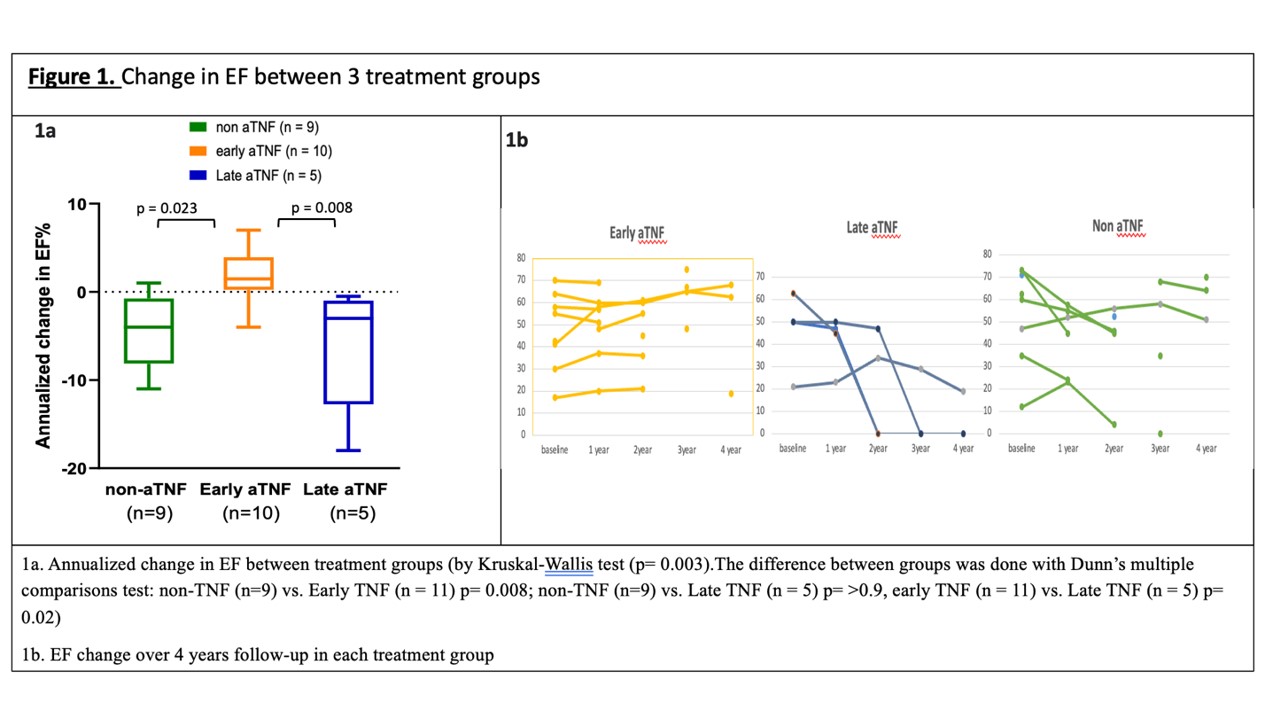
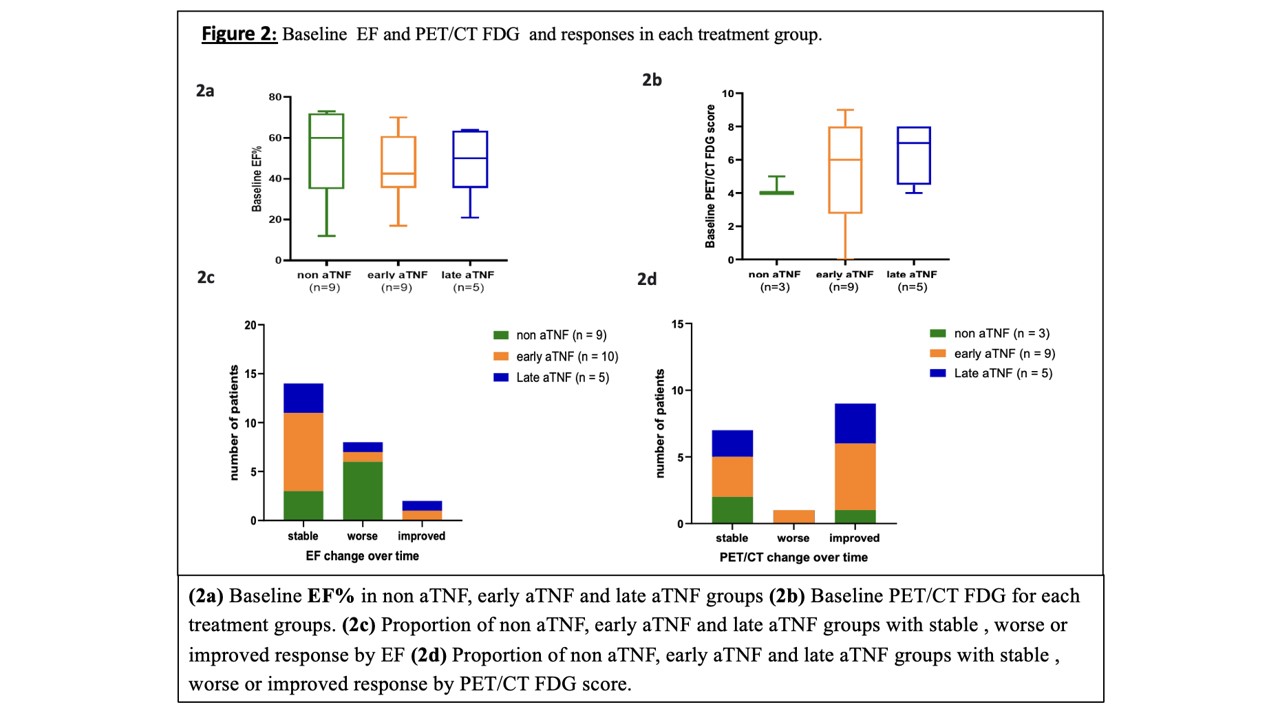
Results: The demographic and clinical characteristics of 29 patients with cardiac sarcoidosis are shown in Table 1. Paired EF analysis was performed on 24 patients with >2 follow-up EF including 2 reassigned to non aTNF group. In paired PET analysis, 17 patients with >2 PET scans were included. Survival was similar for all groups, 80% (8/10) in non-aTNF, 86% (6/7) in late aTNF and 92% (11/12) in early aTNF. In the non aTNF group, 4 patients received a cardiac transplant. Most patients with RV involvement were in the early aTNF group (7/12; 58%), vs the non aTNF (1/10; 10%) and late aTNF (2/7; 29%) (p = 0.06) Table 1. There was no difference between groups in baseline EF (p = 0.9) and PET score (p = 0.07) (Fig 2). Annualized EF improvement in early aTNF was significantly higher compared to late aTNF group (p = 0.02) and non aTNF group (p = 0.008) with no difference between the non aTNF and late aTNF groups (p = 0.9) Figure 1a. Although the time for follow-up varied among patients, 1/10 (10%) early aTNF patients had >10% EF decline compared to 6/9 (67%) non aTNF and 2/5 (40%) late aTNF patients but the time of follow-up varied between patients. Improvement in PET score was seen in 5/9 (56%) early aTNF, 3/5 (60%) late aTNF and 1/3 (33%) in non aTNF group Figure 2 c,d. At baseline, 8/12 (67%) early aTNF patients were on 7mg (SD7.17) daily prednisone dose, 4/7 (57%) late TNF patients were on 19mg (SD 22.68), and 7/10 (70%) non aTNF were on 25mg (SD 21.21). Over time 20% (2/10) of non aTNF were at a higher dose than baseline compared to 10% (1/10) of the early aTNF and 16% (1/6) of late aTNF groups.
Conclusion: In this cohort, early aTNF use was associated with improvement in yearly EF change compared to none or late users, suggesting prescribing aTNF early may be associated with EF protection. Slightly higher proportions of non and late aTNF remained on steroids compared to early aTNF. Further research on use and timing of aTNF in cardiac sarcoidosis is warranted.
To cite this abstract in AMA style:
Singh K, Zucker H, Kwon A, Liu A, Rini J, Katzap E, Narain S, Marder G. Treatment Outcomes of TNF-α Inhibitors in Cardiac Sarcoidosis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/treatment-outcomes-of-tnf-%ce%b1-inhibitors-in-cardiac-sarcoidosis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/treatment-outcomes-of-tnf-%ce%b1-inhibitors-in-cardiac-sarcoidosis/