Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: In the treatment and follow-up of rheumatoid arthritis (RA) patients, it has become more desirable to detect changes in disease activity through remote monitoring. Patient reported outcomes(PROs) might be useful for this purpose. So far associations between PROs and changes in disease activity have been mostly investigated on a continuous scale. However, in daily practice, and in line with the current recommendations, treatment decisions are mainly based on the patient’s disease activity status. Earlier literature has shown that functionality, morning stiffness, health-related quality of life (HRQoL), general health (GH), joint pain and fatigue change with the development and resolution of a disease flare.
Therefore, our aim is to determine if PROs that cover functionality, joint pain, morning stiffness, HRQoL, GH and fatigue are sensitive to disease activity status alterations in patients with early and established RA.
Methods: Early RA patients from the tREACH trial and established RA patients from the TARA trial were included. Both studies are multicentre, single-blinded trials with a treat-to-target approach. Treatment alterations were based on the disease activity score (DAS44) and PROs were collected at 3-montly intervals. The following PROs were studied: (1) the Health Assessment Questionnaire-Disability Index(HAQ-DI), (2) morning stiffness severity (numeric rating scale, NRS 0-10), (3) the 3-level EQ-5D(EQ-5D-3L) (4) GH (visual analogue scale, VAS 0-100mm), (5) joint pain (NRS 0-10) and (6) fatigue (VAS 0-100mm).
Disease activity status were defined as: (1) active disease (DAS≥2.4), (2) low disease activity (LDA, DAS< 2.4 and ≥1.6), and (3) remission (DAS< 1.6). Differences in disease activity status between two consecutive visits were compared to changes in PROs. Mean changes in PROs per disease activity status alteration were compared to stable disease activity status using linear mixed models.
Results: A total of 587 early and 189 established RA patients were included. The median symptom duration (interquartile range, IQR) was 0.4 (0.2-0.6) and 6.2 (4.1-8.9) years respectively. The mean DAS (95% confidence interval, CI) at baseline was 3.0 (3.0-3.2) in the early and 1.0 (0.9-1.1) in the established RA group.
Figure 1 shows the mean change in PROs per change in disease activity status(with 95%CI and significance). Changes in HAQ-DI, morning stiffness severity, EQ-5D-3L, GH, joint pain and fatigue (in early RA) were in concordance with improvement or worsening of the disease activity status. Changes from remission or LDA to active disease and vice versa had a bigger impact on the change in PRO compared to changes between LDA and remission.
Conclusion: HAQ-DI, morning stiffness, EQ-5D-3L, GH and joint pain are sensitive to changes in disease activity status. These results suggest that aforementioned PROs may be helpful in remote monitoring of RA.
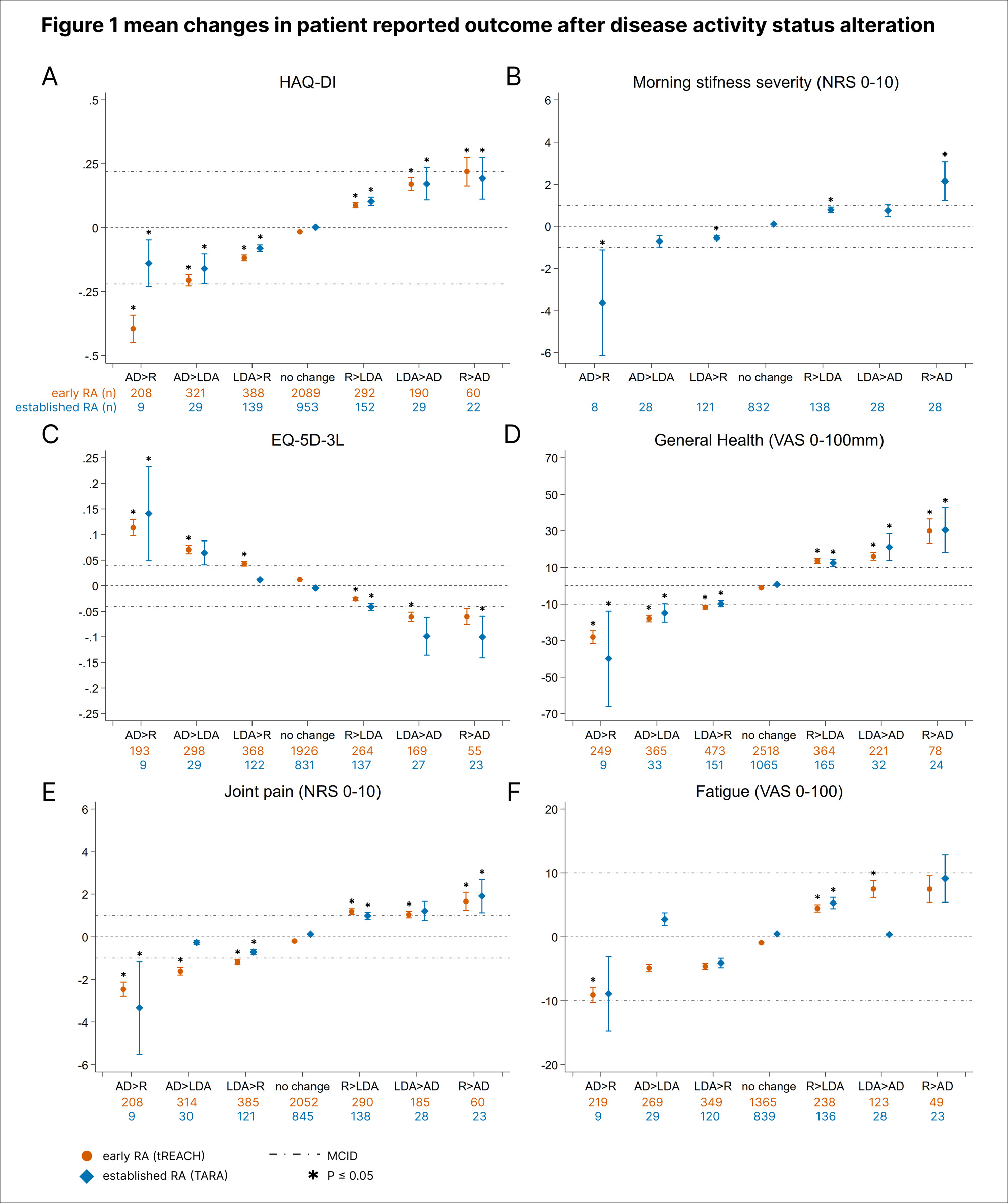
Abbreviations: AD, active disease; EQ-5D_3L, 3-level EQ-5D; HAQ-DI, health assessment questionnaire-disability index; LDA, low disease activity; NRS, numeric rating scale; R, remission; VAS, visual analogue scale.
To cite this abstract in AMA style:
Loiojen A, van Mulligen E, van der Helm-van Mil A, de Jong P. Towards a Guide for Evidence-based Remote Monitoring: Sensitivity of Patient Reported Outcomes to Change in Disease Activity Status in Early and Established Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/towards-a-guide-for-evidence-based-remote-monitoring-sensitivity-of-patient-reported-outcomes-to-change-in-disease-activity-status-in-early-and-established-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/towards-a-guide-for-evidence-based-remote-monitoring-sensitivity-of-patient-reported-outcomes-to-change-in-disease-activity-status-in-early-and-established-rheumatoid-arthritis/