Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The management of juvenile dermatomyositis (JDM) is not standardized and no widely embraced therapeutic protocols are available. Furthermore, the optimal therapeutic targets as well as the ideal timing of their achievement are not established. Defining these aspects of the therapeutic approach would be fundamental to implement the treat-to-target (T2T) strategy. The aim of the present project was to investigate the longitudinal trends of indicators of treatment effectiveness in a cohort of JDM patients, with the aim of identifying suitable targets and optimal timing of their achievement.
Methods: We reviewed retrospectively the charts of 44 patients diagnosed with JDM, seen at our center within 6 months after disease diagnosis and followed for ≥ 6 months. The disease course was assessed at the following time points: baseline (diagnosis) and after 1.5, 3, 6, 12, 18 and 24 months. Collected data included demographic features, muscle enzymes, and the main physician- and parent-centered JDM outcome measures. Time to skin and muscle remission, normalization of muscle enzymes, inactive disease (ID) by PRINTO modified criteria, complete clinical response (CCR), ID by JDMAI1 and JDMAI2, reduction of prednisone (PDN) dose < 0.3 mg/kg/day and < 0.1 mg/kg/day, and glucocorticoid (GC) discontinuation was calculated. Treatment response by IMACS and PRINTO criteria, as well as longitudinal changes in JDMAI1 and JDMAI2 were also evaluated.
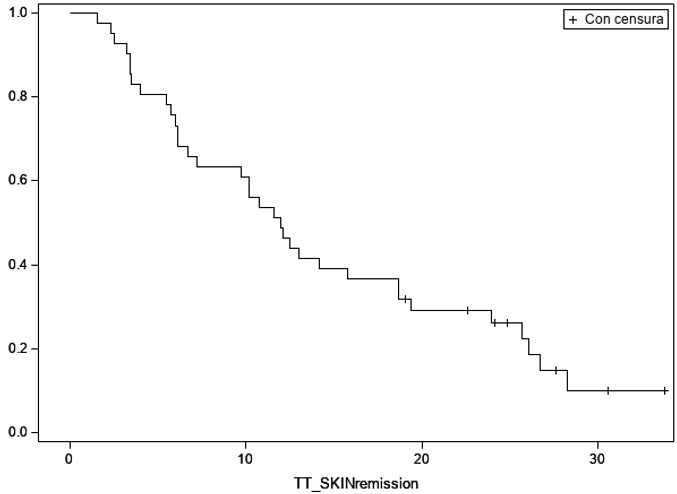
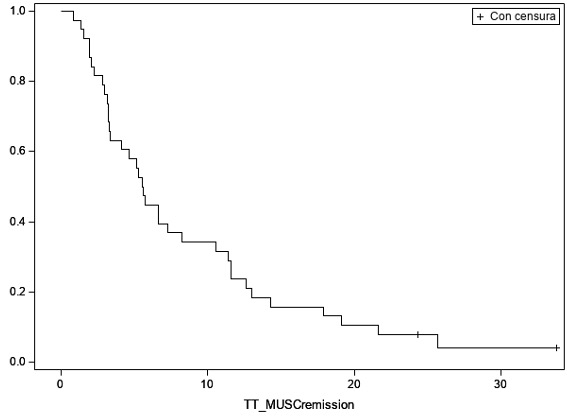
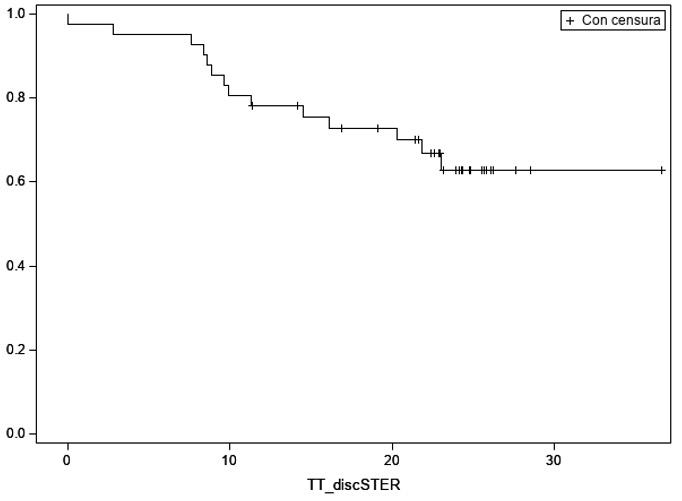
Results: A total of 44 patients (median age at diagnosis 7.5 years; median time from onset to diagnosis 4.2 months) were included. All but 4 patients received high-dose GC at diagnosis, associated with methotrexate and IVIG in 64% and 20.5%, respectively. The frequency of and median time to achievement of established targets were: 82.9% and 12.0 months for skin remission (Figure 1); 94.7% and 5.6 months for muscle remission (Figure 2); 94.1% and 3.0 months for normalization of muscle enzymes; 79.5% and 13.0 months for ID by PRINTO modified criteria; 68.2% and 18.6 months for CCR; 60% and 13.0 months for ID by JDMAI1; 64% and 12.9 months for ID by JDMAI2; 100% and 11.2 months for PDN dose reduction to < 0.3 mg/kg/day; and 56.1% and 24.7 months for PDN dose reduction to < 0.1 mg/kg/day. GC were discontinued in 34.1% patients (median time not reached) (Figure 3). IMACS minimal/moderate/major improvement was reached in 36.4%/56.8%/40.9% of patients, whereas PRINTO minimal/moderate/major improvement in 32%/76%/52%, respectively. JDMAI1 and JDMAI2 scores declined over time, especially at 12 months (mean absolute/percentage change from baseline: -14.1/-90.0% for JDMAI1, -14.7/-84.4% for JDMAI2).
Conclusion: Our findings provide preliminary figures derived from the real world of clinical practice that may help to define suitable targets and optimal timing of their achievement for the future introduction of the T2T strategy in JDM.
To cite this abstract in AMA style:
Rosina S, Rebollo-Giménez A, Campone C, Natoli V, Consolaro A, Bovis F, Ravelli A. Toward a Treat-to-target Strategy in Juvenile Dermatomyositis: Seeking for Suitable Targets and Optimal Timing of Their Achievement [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/toward-a-treat-to-target-strategy-in-juvenile-dermatomyositis-seeking-for-suitable-targets-and-optimal-timing-of-their-achievement/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/toward-a-treat-to-target-strategy-in-juvenile-dermatomyositis-seeking-for-suitable-targets-and-optimal-timing-of-their-achievement/