Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: The diagnostic gold standard of the diagnosis of gout is joint aspiration and the identification of monosodium urate (MSU) crystals under polarized light microscopy. However, arthrocentesis is not always a viable option, for example if there is no effusion on exam or an adequate sample cannot be obtained. Dual-energy computed tomography (DECT), an x-ray-based imaging technique, is a noninvasive diagnostic approach to detect MSU crystals in joints and periarticular tissues. The 2015 American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) classification criteria for gout recognize a role for DECT in the diagnosis of gout. In our retrospective study, we analyzed how DECT was utilized in a cohort of patients at the University of Cincinnati Medical Center in Cincinnati, Ohio.
Methods: The cohort in our retrospective study was screened by identifying patients who had DECT scans performed from November 2013 to May 2022 using radiology software read by two board certified, fellowship trained radiologists with expertise in musculoskeletal imaging. Subsequent charts of patients who also had joint aspirations were then reviewed further. Descriptive statistics, sensitivity, specificity, positive and negative predictive values, and accuracy were calculated.
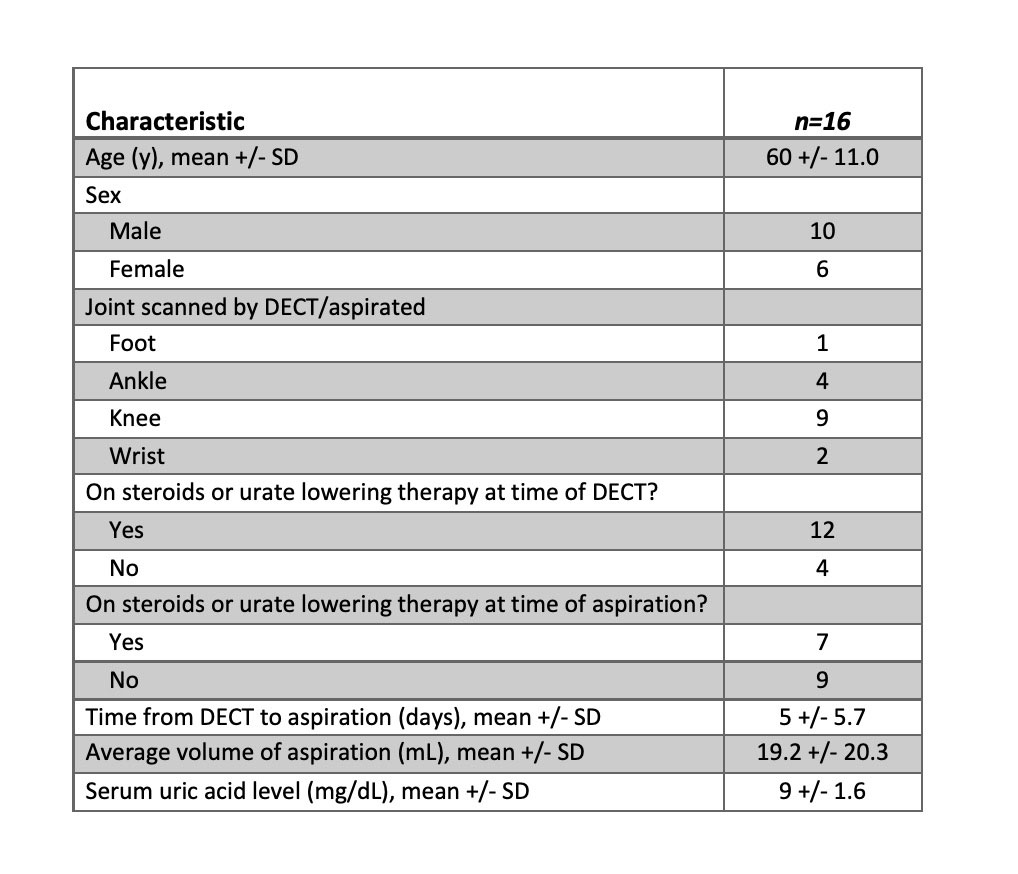
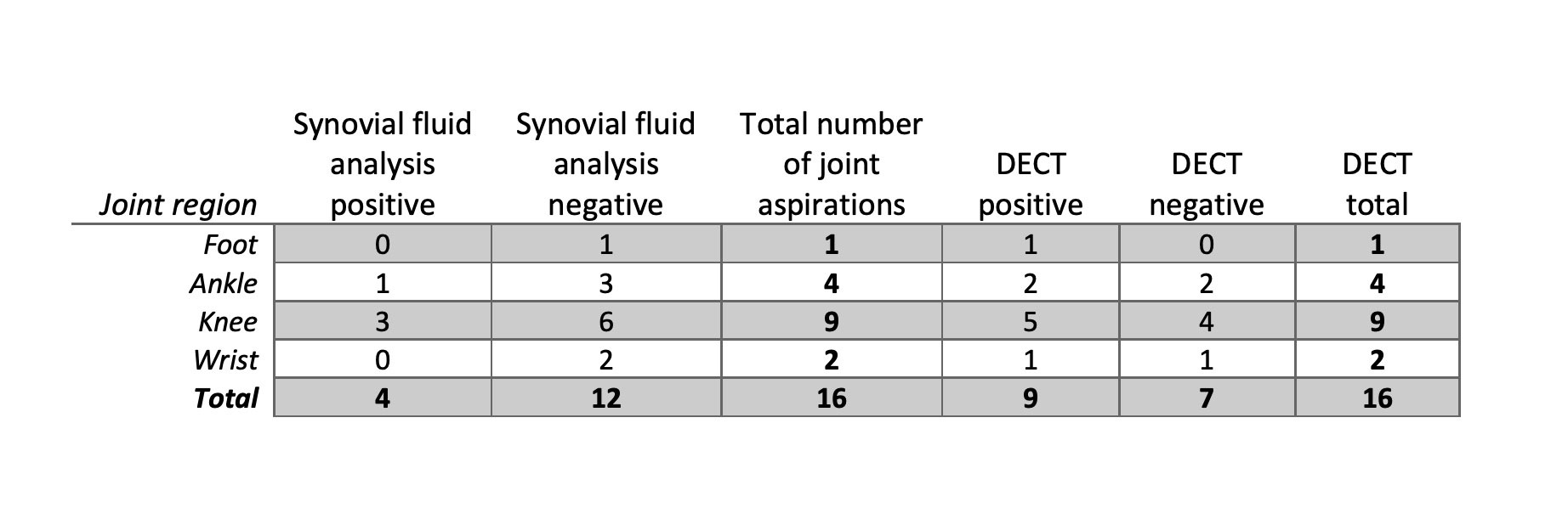
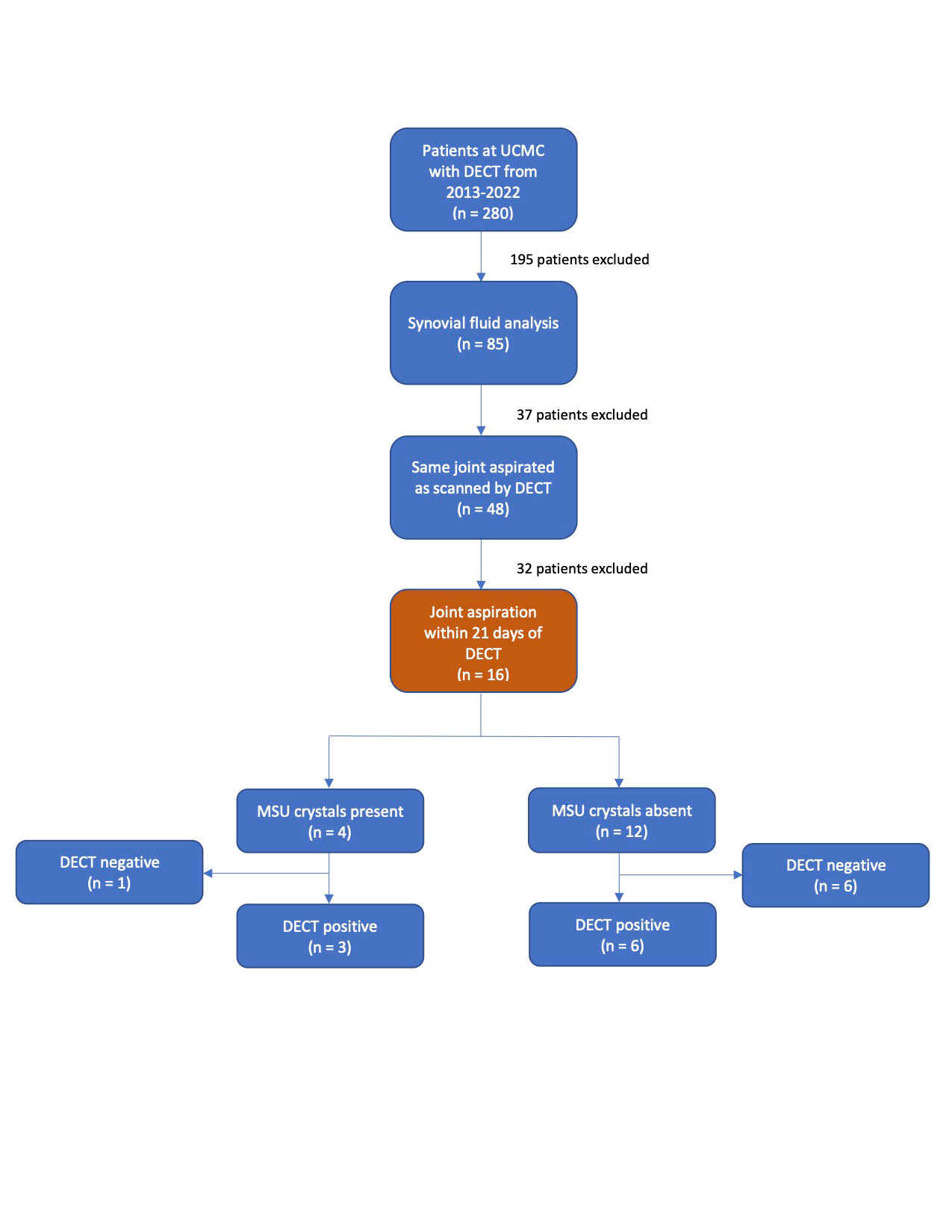
Results: A total of 280 DECT scans were ordered over the observation period. Arthrocentesis was done on 48 of these patients on the same joint that was scanned by DECT. Patients with joint aspirations performed more than 21 days before DECT were excluded from the study, leaving 16 patients who were analyzed (Figure 1). The mean (SD) age was 60 (+/- 11.0). 10 patients were male, and 6 were female (Table 1). The mean (SD) time from DECT to aspiration was 5 days (+/- 5.7). 4 of 16 patients had MSU crystals present on aspiration, of which 3 of these patients had a positive DECT scan. 12 of the 16 patients had no MSU crystals present on aspiration, of which 6 had a positive DECT scan. Two patients had a negative fluid analysis and underwent repeat arthrocentesis within a 21-day period which identified MSU crystals (Table 2). The sensitivity of DECT in diagnosing gout, using positive MSU crystals on aspiration as the gold standard, was 75%. The specificity was 50%, negative predictive value was 0.86, and the positive predictive value was 0.33. The accuracy was calculated to be 0.56. When DECT was considered the standard of reference, then joint aspiration for the diagnosis of gout was 33% sensitive and 86% specific with a 75% positive predictive value and 50% negative predictive value.
Conclusion: The utilization of DECT in the diagnosis of gout has recently emerged as beneficial due to its noninvasive, accessible nature. Using joint aspiration as a gold standard, DECT has value in excluding gout with a high negative predictive value. Alternatively, when using DECT as a gold standard, joint aspiration shows low sensitivity but high positive predictive value. Although the cohort of this study was small, these findings indicate an evolving role for DECT in the evaluation of gout perhaps when integrated after a negative joint aspiration.
To cite this abstract in AMA style:
Parikh P, Nguyen K, Vashisht P, Reed C, Jacobson J. The Utility of Dual-Energy Computed Tomography in the Diagnosis of Gout [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/the-utility-of-dual-energy-computed-tomography-in-the-diagnosis-of-gout/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-utility-of-dual-energy-computed-tomography-in-the-diagnosis-of-gout/