Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients with RA are at increased risk of atherosclerotic cardiovascular disease (ASCVD), yet traditional 10-year CVD risk calculators—such as the 2013 Pooled Cohort Equations (PCE)—tend to underperform in RA. The American Heart Association recently published the Predicting Risk of CVD EVENTs (PREVENT) algorithm, an updated risk calculator which expands the age range, excludes race, and includes additional variables relevant to cardiovascular-kidney-metabolic conditions such as BMI, estimated glomerular filtration rate, and optionally the urine albumin-to-creatinine ratio (uACR). We determined the performance of the PCE vs. PREVENT algorithm in predicting subclinical coronary and carotid atherosclerosis in RA.
Methods: Patients fulfilling 1987 ACR RA criteria without known CVD underwent multidetector row CT scanning of the chest, and the Agatston method was used to quantify a coronary artery calcium (CAC) score. They also underwent bilateral carotid artery ultrasound to determine presence of carotid artery plaque, classified as any plaques with ≥25% occlusion of the vessel lumen. The PCE score and three separate 10-year PREVENT scores—total CVD, ASCVD, and total CVD + uACR—were calculated; scores were compared in their performance to indicate CAC (any calcium, CAC ≥100, and CAC ≥300) and the presence of carotid plaque.
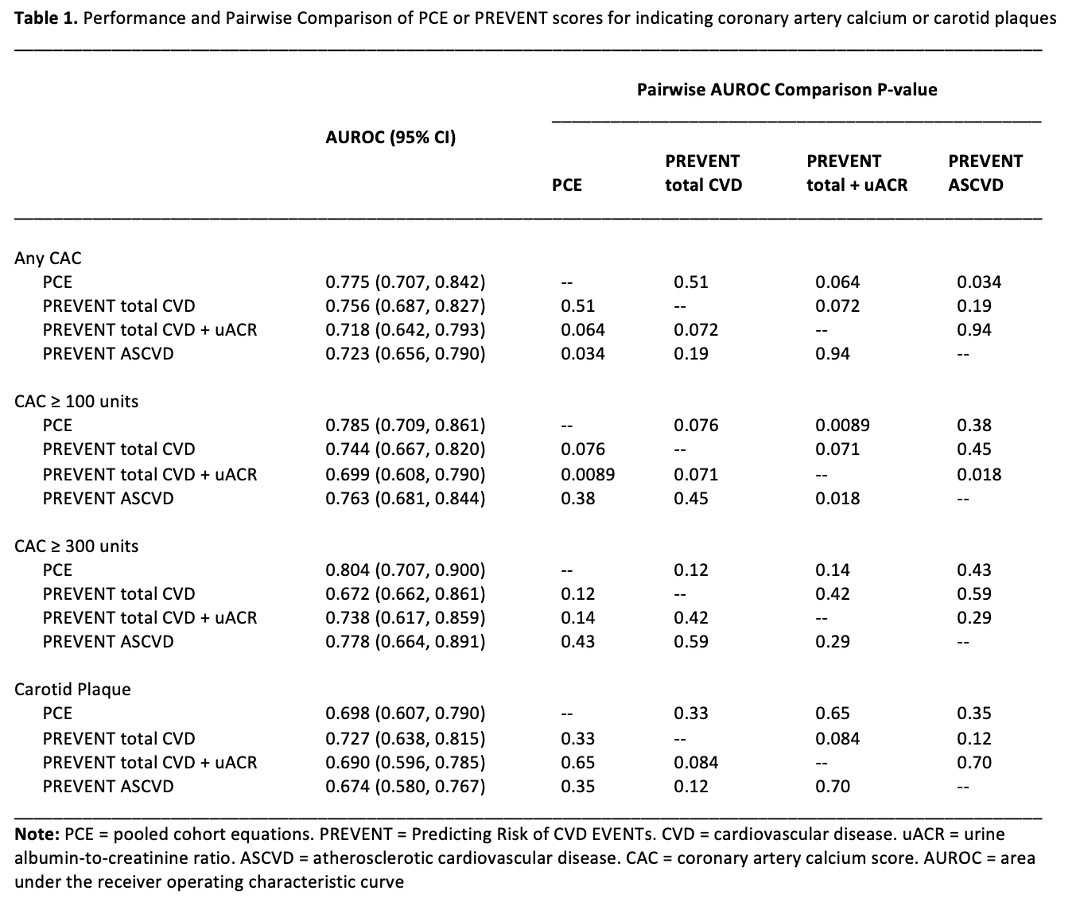
Results: A total of 161 RA patients were included, with a mean age of 59 years and median RA duration of 9 years; 65% were female. Patients had no known CVD or diabetes and were not treated with lipid-lowering medication. Hypertension was present in 50% of patients; the mean total cholesterol was 199 mg/dL and the mean LDL-C was 119 mg/dL. The median PCE score was 5.2%. The median PREVENT algorithm total CVD, total CVD + uACR, and ASCVD scores were 6.7%, 5.8%, and 3.7%, respectively. The PCE score was significantly different from each of the PREVENT scores (p< 0.001 for each comparison). We compared the stratification of patients by each algorithm into 10-year risk groups based on predicted probability of ASCVD: low risk (< 5%), borderline risk (5-7.49%), intermediate risk (7.5-19.9%), and high risk (≥20%); the PCE and PREVENT scores were concordant in 67% of patients for the total CVD score, 62% for the total CVD + uACR score, and 59% for the ASCVD score. The PCE and all of the PREVENT scores were robustly and significantly associated with all levels of CAC and presence of carotid plaque. For all levels of CAC, the PCE had the highest area under the receiver operating characteristic curve (AUROC), which was not significantly different from the PREVENT total CVD scores (Table 1). The addition of uACR did not improve the prediction of subclinical ASCVD. For carotid plaque, the PREVENT total CVD score had the highest AUROC, though the AUROC curves for all the scores were not significantly different.
Conclusion: The newly-updated PREVENT scores for CVD risk were not better than the prior PCE algorithm for indicating subclinical coronary and carotid atherosclerosis in RA, which are known predictors of future cardiovascular events. Because the PCE score already underperforms in RA patients, it seems unlikely that the PREVENT algorithm will adequately predict CVD event risk in this population.
To cite this abstract in AMA style:
Gibbons J, Bathon J, Giles J. The Updated PREVENT (Predicting Risk of CVD EVENTs) Algorithm Is Not Able to Indicate Subclinical Coronary or Carotid Atherosclerosis Better Than the Traditional Pooled Cohort Equations in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/the-updated-prevent-predicting-risk-of-cvd-events-algorithm-is-not-able-to-indicate-subclinical-coronary-or-carotid-atherosclerosis-better-than-the-traditional-pooled-cohort-equations-in-rheumatoid/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-updated-prevent-predicting-risk-of-cvd-events-algorithm-is-not-able-to-indicate-subclinical-coronary-or-carotid-atherosclerosis-better-than-the-traditional-pooled-cohort-equations-in-rheumatoid/