Session Information
Date: Sunday, November 17, 2024
Title: Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
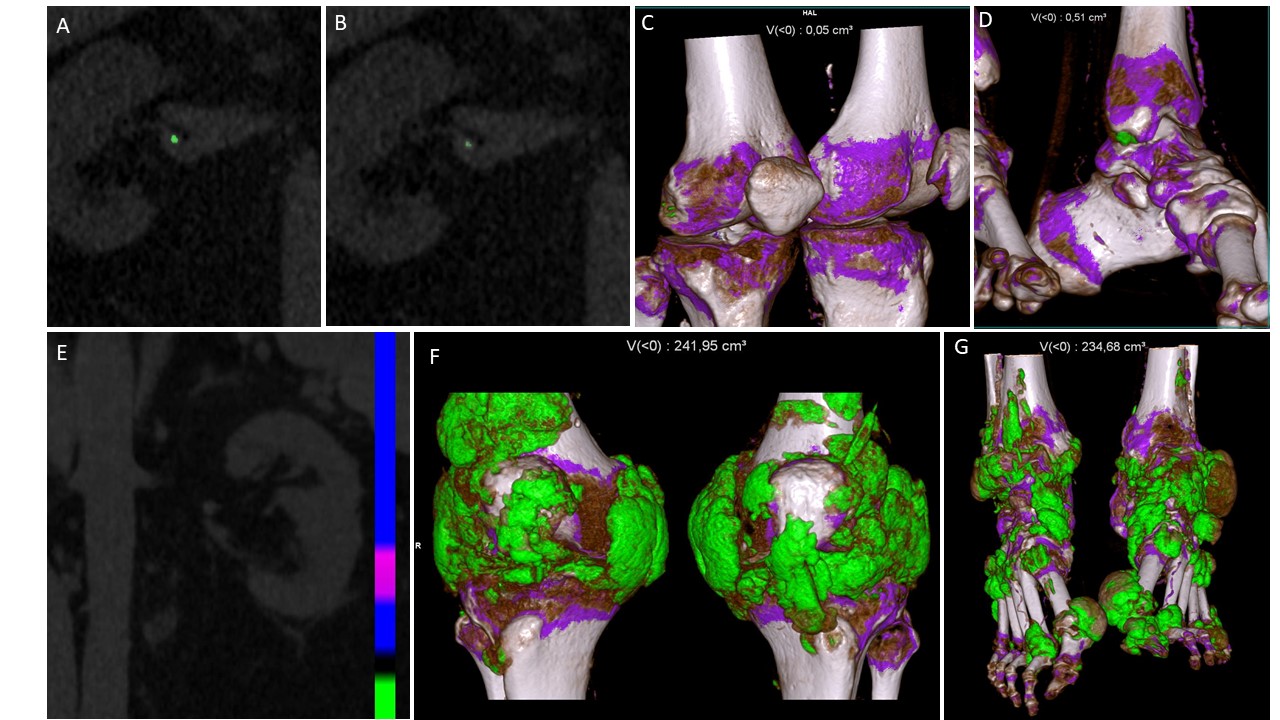
Background/Purpose: Chronic kidney disease (CKD) is a common feature in gout, and can have multiple causes, some of which are gout specific, such as gout nephropathy (deposition of monosodium urate (MSU) crystal in the renal medulla), due to chronic uric acid urolithiasis, or vascular nephropathy related to debated arterial MSU plaques. Dual-energy CT (DECT) has been extensively demonstrated to identify MSU crystal deposition around joints, but its ability to detect MSU crystals in kidney and vessel walls is unclear. The objective of this study was to explore if DECT can detect MSU crystal deposits in the renal medulla and renal artery walls, and uric acid urolithiasis, in patients with gout and CKD.
Methods: Patients with gout according to the 2015 ACR/EULAR classification criteria and with stage 2-4 CKD were prospectively included in this exploratory cross-sectional study. Patients’ demographics, comorbidities, gout characteristics and treatment, current serum urate (SU) levels and estimated glomerular filtration rates (eGFR) were recorded. Patients underwent renal, knee and feet DECT scans. Volumes of MSU crystal deposition at the knees and feet were measured. Renal DECT scans were read for >2mm MSU-coded lesions in the renal tissue, renal artery walls, and urinary tract using first ‘gout’ default settings, then with optimized settings, and finally with the ‘kidney stones’ settings. Presence of renal artery calcifications were noted. Characteristics of patients with and without lesions coded as MSU or uric acid in the renal tissue, renal artery walls and urinary tract were compared.
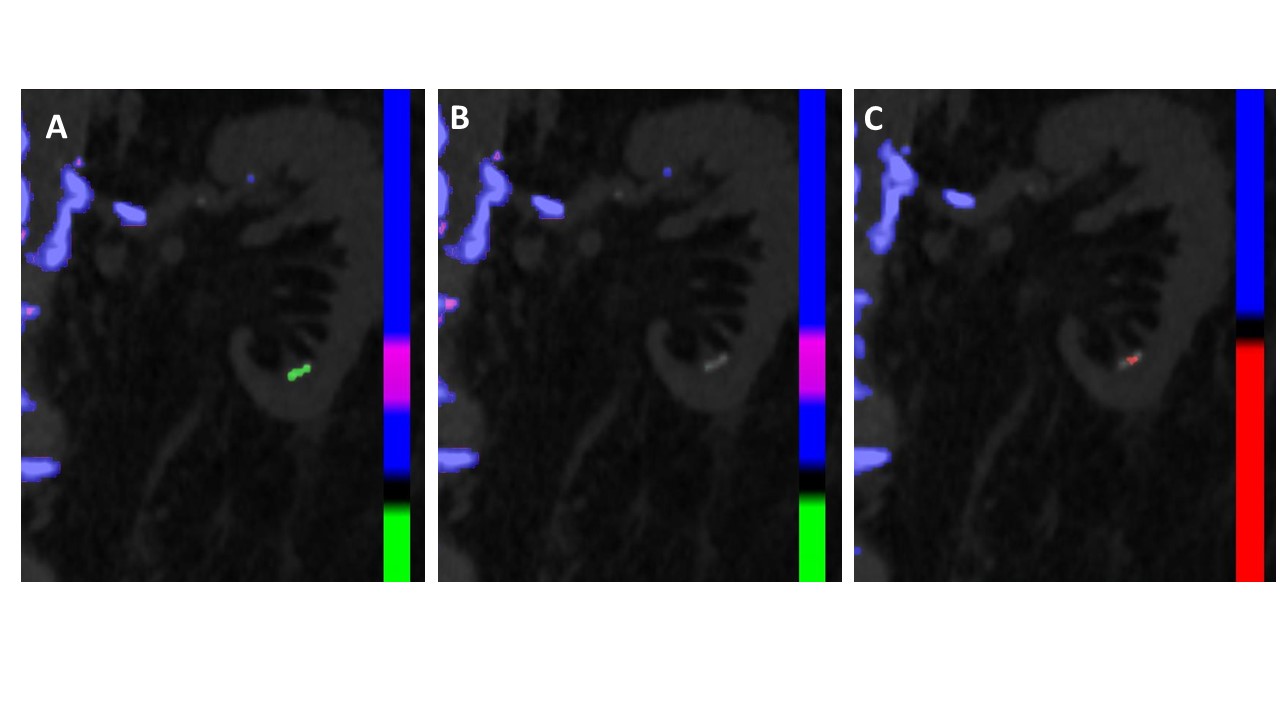
Results: A total of 27/31 patients underwent renal DECT scans and were included in the analysis (23/27 men, mean (SD) 73 (9) years old). Gout duration was 5 [2;7] years and current SU levels were 9.2 (3.1) mg/dL. A total of 19/27 (70.4%) patients had positive knee and feet DECT scans for MSU crystal deposition (cumulative volumes ranging from 0.11 to 475.0 cm3). Mean eGFR was 45.3 ml/min/1.73m2 (21.0), and renal artery calcifications were observed in 21/27 (77.8%) patients. None of the patients exhibited deposition of MSU crystal in the renal tissue (Figure 1). One caliceal lithiasis was observed, coded as MSU crystals in ‘gout’ default settings, disappeared with ‘gout’ optimized settings, and was coded as uric acid in the ‘kidney stone’ settings (Figure 2). Four patients had MSU-coded plaques both in default and stringent ‘gout’ settings in renal arteries, one of them also coded as uric acid in the ‘kidney stones’ settings. Arterial MSU-coded plaques were associated with younger age (66 vs 75 years), higher SU levels (11.5 (3.2) mg/dL vs 8.7 (2.9)), higher eGFR (69.1 (19.0) ml/min/1.73m2 vs 42.7 (20.8), and had similar volumes of MSU deposits in knees and feet. MSU-coded plaques were systematically associated with renal artery calcifications.
Conclusion: DECT was not able to detect evidence of gout nephropathy, even in patients with extensive MSU crystal deposition around joints. DECT can detect uric acid urolithiasis, miscoded as MSU in ‘gout’ default settings. DECT identifies MSU-coded plaques in renal arteries, unrelated to the general MSU crystal burden, most probably miscoded due to calcified plaques.
To cite this abstract in AMA style:
Pascart T, Dauphin E, Yokose C, Jauffret C, Choi H, Budzik J. The Role of Renal Dual-Energy CT in Exploring the Gouty Kidney: The RENODECT Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/the-role-of-renal-dual-energy-ct-in-exploring-the-gouty-kidney-the-renodect-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-role-of-renal-dual-energy-ct-in-exploring-the-gouty-kidney-the-renodect-study/