Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose:
A positive (+)ANA titer is a common reason for Rheumatology consultation, yet the ANA is a nonspecific, non-diagnostic, lab test that is positive in up to 20% of the general population. The goal of this study is to show the low frequency of ANA associated autoimmune diseases (AD) in patients referred for a +ANA, and that low titer ANA are not helpful in diagnosing AD.
Methods:
This was a retrospective review of diagnoses from new patient visits (NPV) to Rheumatology from 1/2/2017 to 12/31/2019 for a +ANA (≥40 titer) cited in the referral or in the rheumatology consultative assessment. Diagnoses were categorized as ANA associated autoimmune diseases(AD) (RA, SLE, Sjogrens, Scleroderma, Myositis, Mixed or undifferentiated connective tissue disorder), other rheumatologic diseases (RD), non-rheumatologic inflammatory conditions (IC), musculoskeletal(MSK) and non-MSK signs/symptoms and non-inflammatory MSK conditions. ANA titers associated with the NPV were identified from the electronic health record if performed in house. Descriptive statistics were used to describe the prevalence of diagnoses and ANA titers. A logistic regression model was fitted to predict AD using ANA titer as the sole predictor; the ROC statistic was used to assess the success of the prediction.
Results:
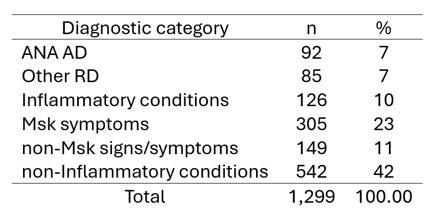
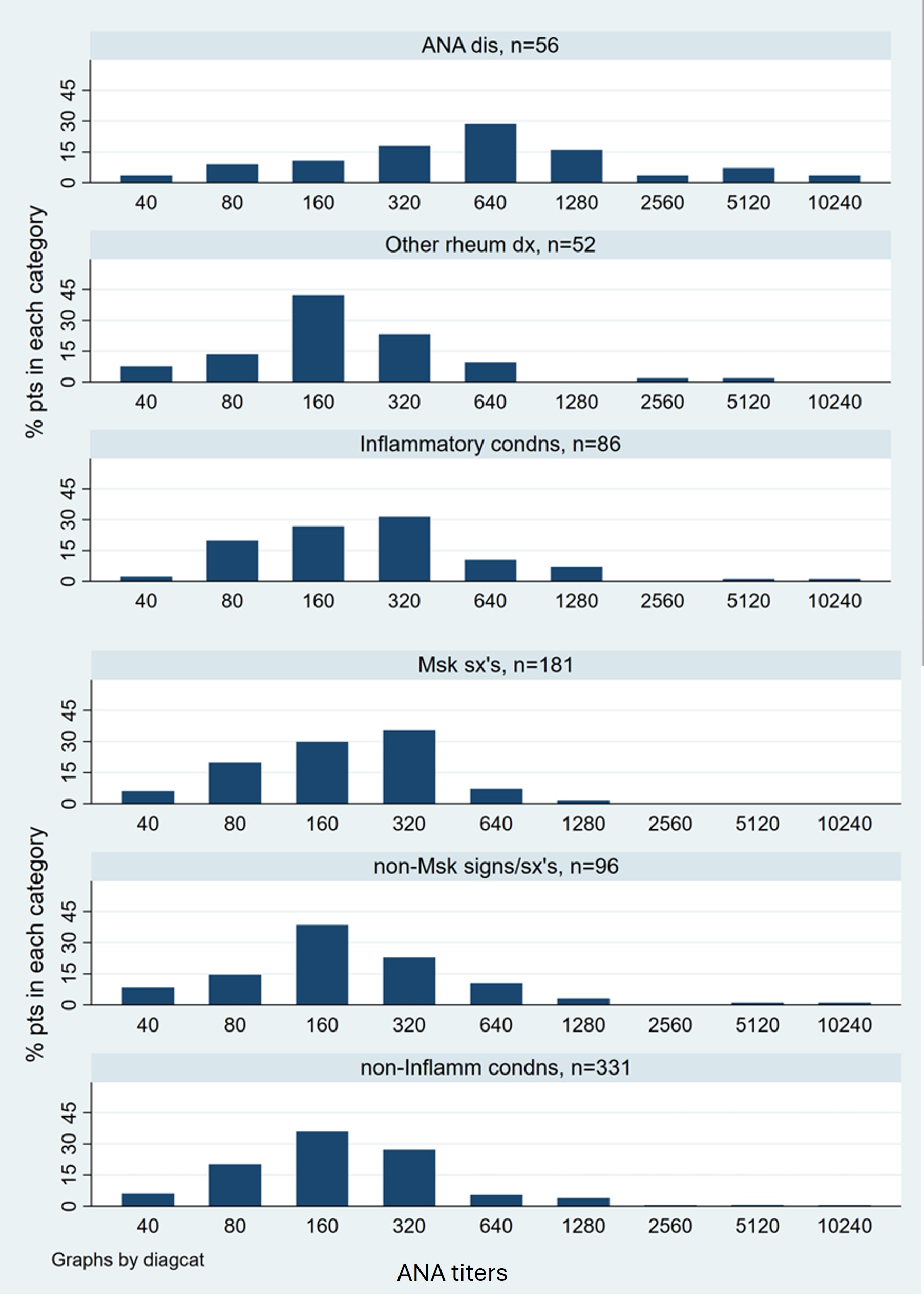
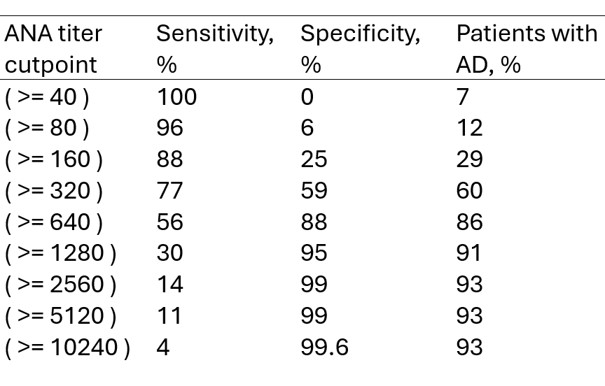
Of 1299 NPV for +ANA, only 7% were diagnosed with AD, 7% with RD, and the rest had no rheumatologic disorder (Table 1). Of 802 patients who had ANA titers documented, 85% had titers ranging from 40 to ≤ 320; the titer distributions were similar amongst the diagnostic categories (Figure 1). The AD group had a higher percentage of ANA titers ≥640, but such high titers were also seen in the groups with nonspecific symptoms or non-inflammatory conditions although less frequently (Figure 1). The specificity for the AD diagnosis was close to 90% for titers ≥ 640, but the sensitivity was only 56% (Table 2). A logistic model showed that ANA titers predicted AD with an acceptable level of discrimination (ROC area of 0.75 [95% CI 0.67, 0.83]).
Conclusion:
Less than 1 in 10 referrals for +ANA were associated with ADs. The prevalence of +ANA titers ≤320 was common in this cohort, and did not distinguish AD from other diseases. ANA titers ≥640 were more specific for AD, but could still be found in non-AD groups. In a general Rheumatology practice, a provider would have to see 33 new patients with +ANA ≤ 320 in order to diagnose one case of AD. A +ANA is a poor predictor of AD at lower titers, and should not be the only reason for Rheumatology referral.
To cite this abstract in AMA style:
Lau C, Arif A. The Relevance of a Positive ANA in New Patient Referrals to Rheumatology [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/the-relevance-of-a-positive-ana-in-new-patient-referrals-to-rheumatology/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-relevance-of-a-positive-ana-in-new-patient-referrals-to-rheumatology/