Session Information
Date: Monday, November 13, 2023
Title: (1264–1307) RA – Diagnosis, Manifestations, and Outcomes Poster II
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Psychosocial factors may interplay with biological factors to drive a refractory disease state in patients with inflammatory arthritis1. We aim to explore which socioeconomic, and disease related factors associated with persistent active rheumatoid arthritis (PactiveRA) in the first year, despite use of conventional synthetic DMARDs.
Methods: NEIAA is an observational cohort of adult patients with early RA patients in England and Wales. Data from May 2018 until Oct 2022 were acquired. All patients fulfilled the ACR/EULAR 2010 criteria for RA. Patients were defined as having PactiveRA based on three consecutive Disease Activity Scores (DAS28) of >3.2 at baseline, three and 12 months of follow up. Controlled RA (contRA) was defined as patients started with high DAS28 >3.2 at baseline then entered remission (DAS28 ≤ 3.2 at the three and 12 month time-points). PactiveRA status was used as the primary outcome variable. Univariable, followed by multivariable analyses stepwise forward logistic regression to explore associations with PactiveRA. Age and gender were included in the models as a priori, with socioeconomic variables handled as the main independent variables (social deprivation, smoking-status and comorbidities) of interest, followed by disease related factors.
Results: A total of 15,626 patients had a diagnosis of RA in NEIAA. Of which, 682 patients with pactiveRA and 1,026 patients with contRA were analysed. Compared to contRA, patients with PactiveRA were younger (aged 58, interquartile range (IQR): 49, 67) vs (62, IQR: 52,72), included more females 471 (69%) vs 607 (59%), were current or ex-smokers, and more likely to have depression, lung and gastrointestinal disease.
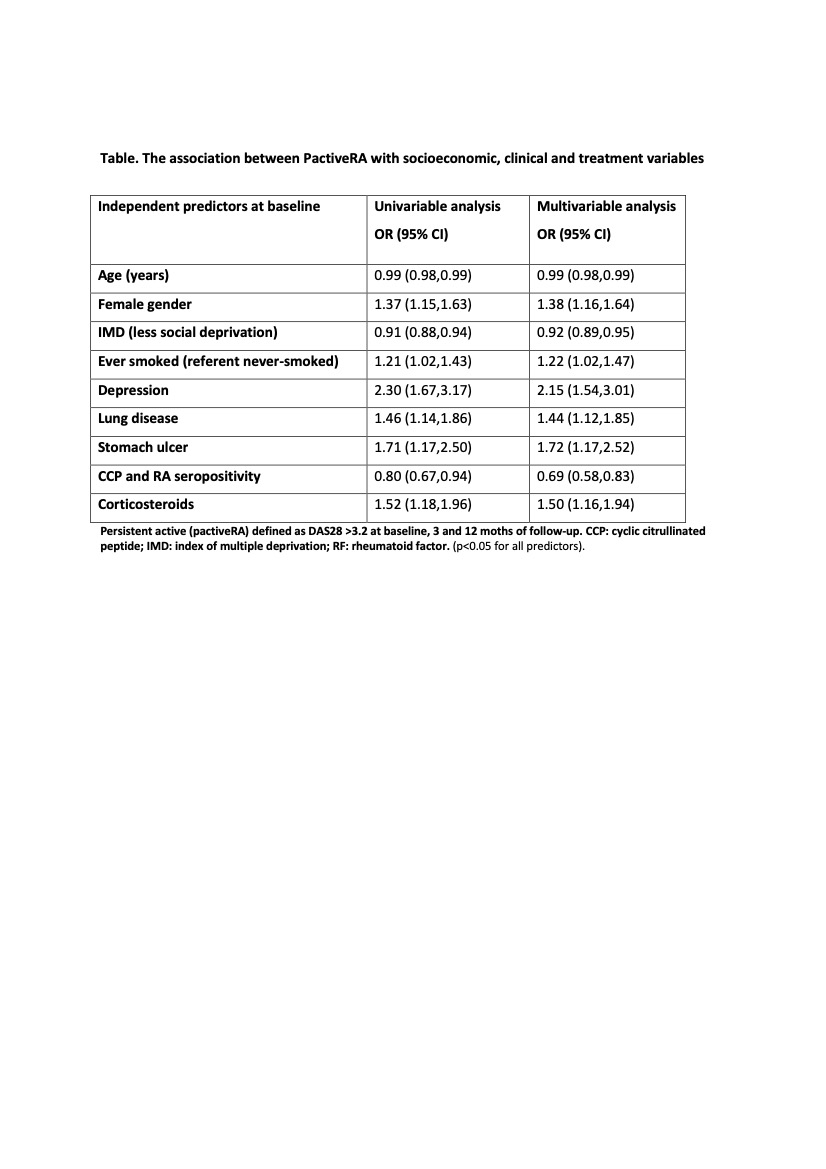
Also, patients with PactiveRA had worse scores in Patient Reported Outcomes at baseline and Patient Health Questionnaire Anxiety and Depression Screener. Logistic regression results are summarised in the table. Age, gender, living in a socially deprived area and being an ex or current smoker, were associated with PactiveRA in models controlling for markers of disease severity (seropositivity). Baseline corticosteroid use was also associated with PactiveRA (p< 0.05 for all) and having a concomitant diagnosis of depression, odds ratio (OR) 2.30 (95%CI: 1.67,3.17), lung disease OR 1.46 (95%CI: 1.14,1.86) and gastric ulcer OR 1.71 (95%CI: 1.17,2.50) were significantly related to PactiveRA.
Conclusion: Sociodemographic factors and living in socially deprived areas were all associated with PactiveRA, independent of clinical and disease characteristics. Identifying ‘adverse’ socioeconomic factors that could drive persistent active disease early in the disease process, can help better guide interventions that would be suitable for individual patients and their respective needs.
To cite this abstract in AMA style:
Adas M, Norton S, Cope A, Buch M, Galloway J, Nikiphorou E. The Relationship Between Socioeconomic Factors and Persistent Active Rheumatoid Arthritis: Results from (NEIAA) a Large UK Cohort of Early Inflammatory Arthritis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/the-relationship-between-socioeconomic-factors-and-persistent-active-rheumatoid-arthritis-results-from-neiaa-a-large-uk-cohort-of-early-inflammatory-arthritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-relationship-between-socioeconomic-factors-and-persistent-active-rheumatoid-arthritis-results-from-neiaa-a-large-uk-cohort-of-early-inflammatory-arthritis/