Session Information
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Ultrasound (US) has emerged as a sensitive method, especially when compared to clinical examination, for evaluating disease activity in Rheumatoid Arthritis (RA). Several studies have shown discrepancies between the physical examination and US in detecting inflammation. In this study, we aimed to understand a) for joints that are tender at baseline, what is the response rate (same joint being non-tender at follow up), according to the presence of Doppler signal positivity at therapy initiation; b) for joints that are not tender at baseline, what is the risk of flare (being tender) at follow up, according to the presence of Doppler signal positivity at the therapy initiation.
Methods: At the ORCHESTRA (Ottawa Rheumatology CompreHEnSive TReatment and Assessment) Clinic RA patients starting a new advanced bDMARD/tsDMARD therapy are assessed using a comprehensive screening process which includes a protocoled US scan. Patients are evaluated in the same clinic three months after new therapy initiation. For this analysis, we included all MCP, PIP and wrist joints of every patient. Analysis was performed on a joint level. Tenderness of the joint as baseline and at follow up were grouped according to having Global OMERACT-EULAR Synovitis Score (GLOESS) grade ³ 2 Doppler signals at baseline. Odds ratio (confidence intervals) were calculated a) for joints that were tender at baseline to understand the prediction of response; b) for joints that were not tender at baseline to understand the prediction on flare.
Results: There were 40 RA patients (70% female) included in the analysis, with 878 joints being analyzed. The median (IQR) tender and swollen joint counts were 8(11) and 7.5(5), respectively, with a DAS28 score of 3.76 (1.58). The mean (SD) age was 60.1(15.6), with a median (IQR) disease duration of 14.5 (21.3) years. Twenty-one patients (52.5%) were bionaive at baseline and 7(17.5%), 4(10%) and 8(20%) patients had failed 1, 2 or ³3 biologic therapies, respectively.
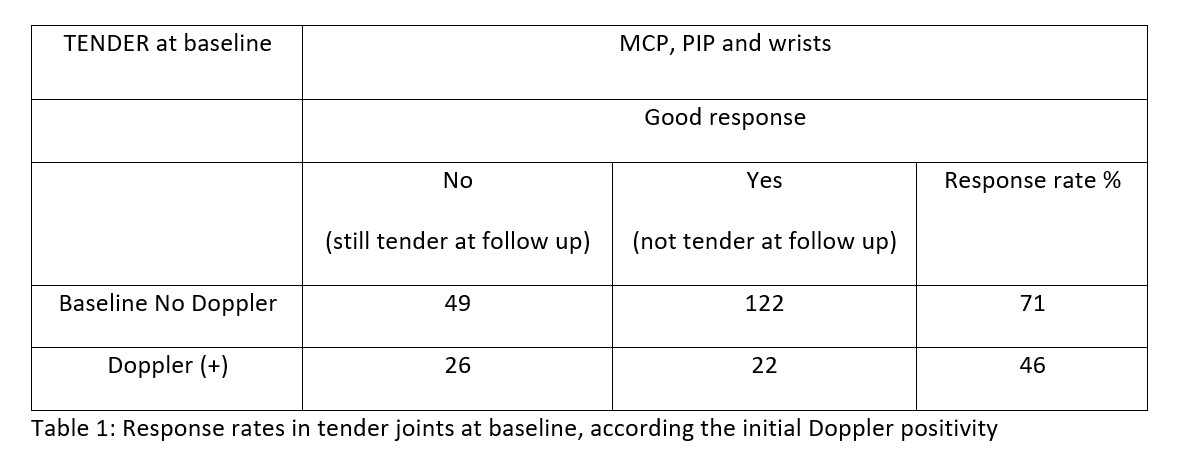
219/878 joints were tender at baseline, 48 (21.9%) of whom had Doppler signals. Among the Doppler positives, the response rate was 46%. The response rate of the joints with no Doppler signals at baseline was 71%, meaning they were no longer tender at follow up. The odds of achieving response on a joint level was lower if there were Doppler signals at baseline (OR 0.34 (CI:0.18-0.66)) (table 1).
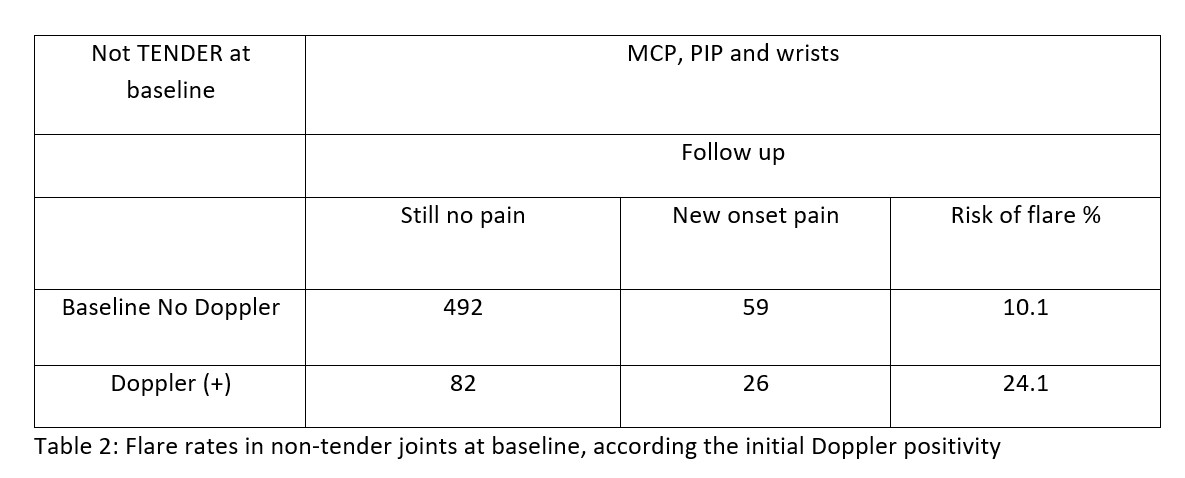
Among the 659 joints that were not tender at baseline, 108 (16.4%) had Doppler signals. Within these, 24.1% became tender at follow up. Among the 551 patients who were Doppler negative, 10.1% became symptomatic. The odds of flaring on a joint level that was previously non-tender was higher if there were Doppler signals at baseline (OR 2.64 (CI:1.58-4.44)) (table 2).
Conclusion: Our study shows that the Doppler signals at the initiation of an advanced therapy has two important meanings on a joint level: Doppler positive tender joints are more resistant to therapies (then Doppler negatives) and Doppler positive non-tender joints have a higher risk of becoming symptomatic. It is still not clear how the US should be incorporated in the treatment algorithms, but the US information suggest a different patient phenotype.
To cite this abstract in AMA style:
Acikgoz S, Gazel U, Sabido-Sauri R, Bayindir Tsechelidis O, Zahrai A, Ivory C, Hepworth E, aydin s. The Prediction of Response to Advanced Therapies on a Joint Level in Rheumatoid Arthritis: The Interpretation of Tenderness and Doppler Ultrasound [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/the-prediction-of-response-to-advanced-therapies-on-a-joint-level-in-rheumatoid-arthritis-the-interpretation-of-tenderness-and-doppler-ultrasound/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-prediction-of-response-to-advanced-therapies-on-a-joint-level-in-rheumatoid-arthritis-the-interpretation-of-tenderness-and-doppler-ultrasound/