Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Our aim was to assess prospectively the clinical features and functional impact of inclusion body myositis (IBM), to identify reliable outcome measures for future trials and to identify prognostic factors of this condition.
Methods: Patients were classified with either probable or definite IBM, according to the Griggs’ criteria (Griggs RC, et al. Ann Neurol 1995;38:705-713) or with clinically defined IBM, according to the Medical Research Council criteria (Hilton-Jones D, et al. Neuromuscul Disord 2010;20:142-147). Clinical data, manual muscle testing (MMT), quantitative muscle testing (QMT) of quadriceps extensors with HUMAC Norm CSMi™ dynamometer and IBM functional rating scale (IBM-FRS) were collected according to a standardised protocol (IBM-Net) at baseline (n=51) and one-year follow-up (n=23, QMT performed in a subgroup of 13 patients). The responsiveness to change of MMT, QMT and IBM-FRS was assessed by calculating the standardized response mean (SRM). Cox-regression analysis was performed to estimate the effect of sex, age at disease onset and previous or current treatment with steroids or immunosuppressants on the time to using a walking stick. Time to using a walking stick was modelled using a Kaplan-Meier curve.
Results: Mean age at disease onset was 58 years (16% before the age of 50). Weakness of quadriceps and finger flexors with sparing of proximal upper limb muscles was the most common presentation. After a median time of 7 years of disease, 63% of patients had lost independent walking ability and needed assistive devices. Twenty-seven patients (53%) reported difficulties with swallowing. IBM was initially misdiagnosed in 50% of cases, the commonest misdiagnosis being polymyositis. MMT, IBM-FRS and quadriceps QMT significantly declined after one year (by 5.2%, 13.8% and 27.9% respectively). QMT of the quadriceps muscle (SRM=1.8) and IBM-FRS (SRM=1.3) were the most sensitive measures of disease progression. Disease onset after 55 years of age (HR=4.1; 95% CI=1.7, 9.8; p=0.001), but not sex or treatment, was predictive of a shorter time to requirement of a walking stick (figure). We detected no differences in disease presentation and progression between clinically and pathologically defined IBM patients.
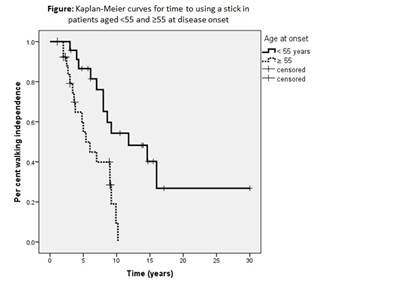
Conclusion: IBM is a disabling myopathy with prominent involvement of specific muscle groups, particularly quadriceps femoris and finger flexors, which are essential for activities of daily living. IBM is still probably an underrecognised and misdiagnosed disease. During one year follow-up, the responsiveness of QMT of quadriceps femoris and of IBM-FRS were greater than MMT, which makes the former two measures more sensitive markers of disease progression. Onset of the disease after 55 years of age was predictive of a shorter time to using a walking stick.
Disclosure:
P. Machado,
None;
A. Cortese,
None;
J. Morrow,
None;
L. Dewar,
None;
A. Hiscock,
None;
A. Miller,
None;
S. Brady,
None;
D. Hilton-Jones,
None;
M. Parton,
None;
M. G. Hanna,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-natural-history-of-sporadic-inclusion-body-myositis-an-observational-longitudinal-study/