Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: The prevalence of childhood-onset SLE (cSLE) differs by racial/ethnic group. Yet, the role of social determinants of health (SDoH) in disease severity is not understood. We hypothesized that in an urban center with a large, diverse catchment area, SDoH influence the severity of cSLE at diagnosis.
Methods: We completed an IRB-approved retrospective review of 136 children newly diagnosed with cSLE between 1/1/18-5/31/22 at Texas Children’s Hospital (TCH). We abstracted demographic, clinical severity characteristics (SLEDAI at diagnosis, inpatient or ICU admission, CNS, CYC therapy) and SDoH variables such as State Area Deprivation Index (ADI; higher quartiles indicate greater deprivation), insurance status, distance to care, pollution burden, food accessibility, and social work consultation. Statistical analyses performed in Stata v15.1 and ArcGIS Pro2.2.
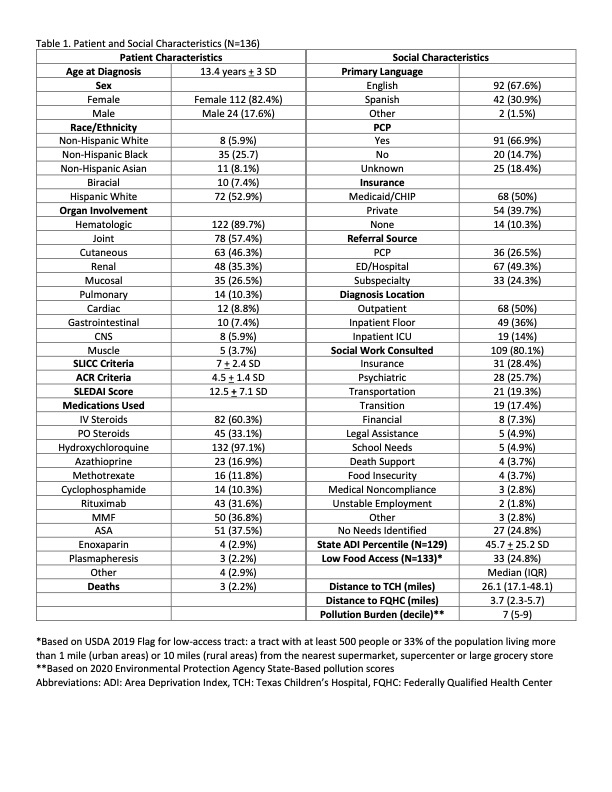
Results: Mean age at diagnosis was 13.4 years + 3 SD, with 82.4% female, 52.9% Hispanic White (HW) and 25.7% non-Hispanic Black (NHB). Fourteen patients (10.3%) were uninsured (UI) and 50% had Medicaid (M) or Children’s Health Insurance Program (CHIP). Half were diagnosed during inpatient admission (14% in the ICU). Average SLEDAI at diagnosis was 12.5 + 7.1 SD; 48.5% had SLEDAI >12 (severe disease). Average ADI (%) was 45.7 + 25.2 SD. Twenty-five percent lived in a census tract with low-access to supermarkets. The median pollution burden score decile was 7 (IQR 5-9). Social work was consulted in 80.1% (Table 1).
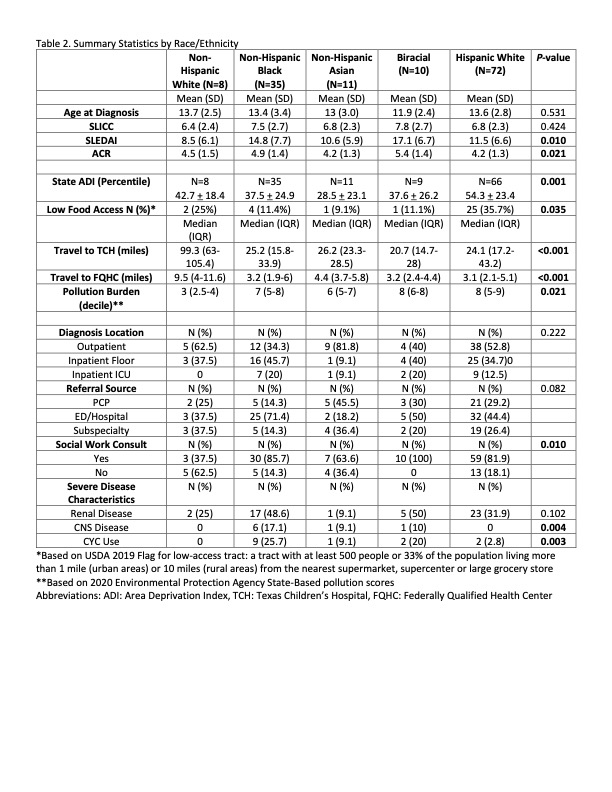
SLEDAI scores were higher in NHB and Biracial (BR) patients at presentation (BR 17.1, NHB 14.8, HW 11.5, Asian (A) 10.6, Non-Hispanic White (NHW) 8.5; P=0.01), Table 2. CNS involvement was highest among NHB children (NHB 17.1%, BR 10%, A 9.1%, HW 0%, NHW 0%; P=0.004). CYC was most often used in NHB and BR patients (NHB 25.7%, BR 20%, A 9.1%, HW 2.8%, NHW 0%; P=0.003). HW patients had the highest ADI (HW 54.3, NHW 42.7, BR 37.6, NHB 37.5, A 28.5; P=0.001) and live in lower food accessible neighborhoods (HW 35.7%, NHW 25%, NHB 11.4%, BR 11.1%, A 9.1%; P=0.035). NHWs travel further to TCH (NHW 99.3 miles, A 26.2, NHB 25.2, HW 24.1, BR 20.7; P< 0.001), live in less polluted neighborhoods (burden score BR 8, HW 8, NHB 7, A 6, NHW 3; P=0.021), and were less likely to have a social work consult (BR 100%, NHB 85.7%, HW 81.9%, A 63.6%, NHW 37.5%; P=0.01).
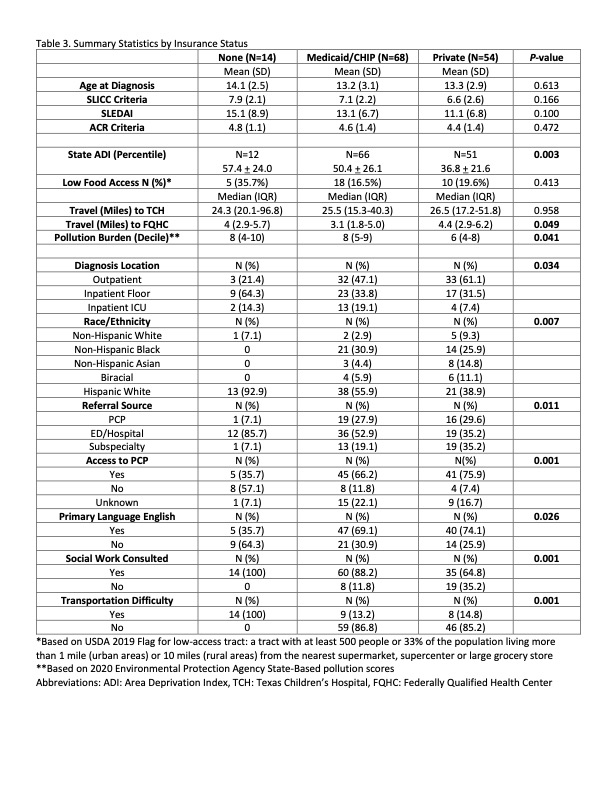
UI patients were most likely to be diagnosed on an inpatient floor and those with M had the highest proportion of ICU admissions (Floor: UI 64.3%, M 33.8%, Private (P) 31.5%; ICU: M 19.1%, UI 14.3%, P 7.4%; P=0.034), Table 3. UI and M patients had higher ADI (UI 57.4%, M 50.4%, P 36.8%; P=0.003), more social work consults (UI 100%, M 88.2%, P 64.8%; P=0.001) and live in more polluted neighborhoods (burden score UI 8, M 8, P 6; P=0.041).
Conclusion: In children with cSLE drawn from a large urban catchment area, we observed an impact of non-modifiable (e.g., race/ethnicity) and modifiable (e.g, insurance status, access to care, food accessibility) factors on disease severity at presentation. Next steps include geospatial mapping to identify high-risk neighborhoods with a discordant number of cSLE patients, and targeting modifiable risk factors in these communities to improve patient experiences and outcomes.
To cite this abstract in AMA style:
Beil E, Muscal E, Oluyomi A, Rosales O, Guffey D, DeGuzman M, Yildirim-Toruner C, Ramirez A, Peckham-Gregory E. The Impact of Social Inequities on Presentation of Childhood-Onset Systemic Lupus Erythematosus (cSLE) at a Large Tertiary Center [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/the-impact-of-social-inequities-on-presentation-of-childhood-onset-systemic-lupus-erythematosus-csle-at-a-large-tertiary-center-2/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-impact-of-social-inequities-on-presentation-of-childhood-onset-systemic-lupus-erythematosus-csle-at-a-large-tertiary-center-2/