Session Information
Date: Saturday, November 12, 2022
Title: RA – Treatment Poster I
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Comorbid conditions may affect efficacy of treatment in patients with rheumatoid arthritis (RA). The aim of this analysis was to evaluate the impact of comorbidity burden on the efficacy of IL-6 inhibitor olokizumab (OKZ) and TNF-α inhibitor adalimumab (ADA) in the CREDO-2 clinical trial cohort of patients with active rheumatoid arthritis (RA).
Methods: Patients in the double-blind RCT (NCT02760407, CREDO-2) received OKZ 64 mg once every 2 weeks (q2w) or 4 weeks (q4w), or ADA 40mg q2w for 24 weeks.
To assess the impact of comorbid conditions on efficacy, outcomes were stratified by patients with Low Charlson Comorbidity Index (CCI = 1; RA only) vs High (CCI ≥ 2; RA and at least 1 comorbidity). Age-points in CCI were excluded since the aim of the analysis was the assessment of comorbidity burden, rather than the mortality prediction.
The comparison of outcomes between the Low and the High CCI groups was performed using χ2-test in unadjusted analysis, and logistic regression in adjusted analysis. Baseline characteristics with an absolute standardized difference > 0.1 were identified as covariates for adjusted comparison. The impact of comorbidity was investigated separately for OKZ and ADA.
The following efficacy parameters were analyzed at Week 12 and Week 24 after the treatment initiation for both ADA and OKZ groups: American College of Rheumatology 20 (ACR20) and 50 (ACR50) responses, proportion of patients achieved Simplified Disease Activity Index (SDAI) ≤ 3.3, Clinical Disease Activity Index (CDAI) ≤ 2.8 and ≤ 10, and Disease Activity Score 28-joint count – C-reactive protein (DAS28(CRP)) ≤ 3.2.
Results: A total of 1402 patients with RA were included to the analysis: 940 patients treated with OKZ 64 mg q2w or q4w (701 (74,6%) with Low CCI and 239 (25,4%) with High CCI) and 462 patients treated with ADA 40mg q2w (352 (76,2%) with Low CCI and 110 (23,8%) with High CCI). All the patients received background MTX therapy.
Gender; age; BMI; smoking status; baseline HAQ Disability Index Score and level of CRP were considered as covariates for the analysis. Additionally, race and alcohol consumption status parameters and duration of RA were considered as covariates for OKZ and ADA analysis, respectively.
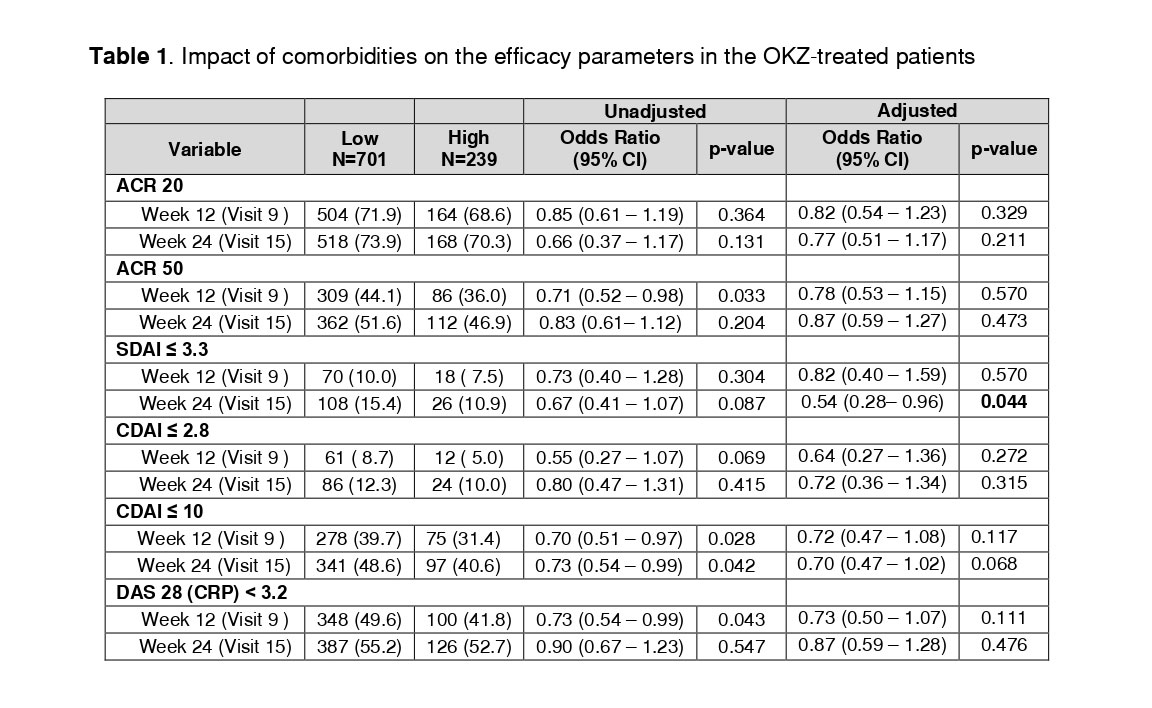
There was no difference in efficacy results between OKZ-treated groups of RA patients with and without comorbid conditions during the study (Table 1), except the achievement of SDAI ≤ 3.3 at Week 24, which was observed more frequently in the Low CCI group.
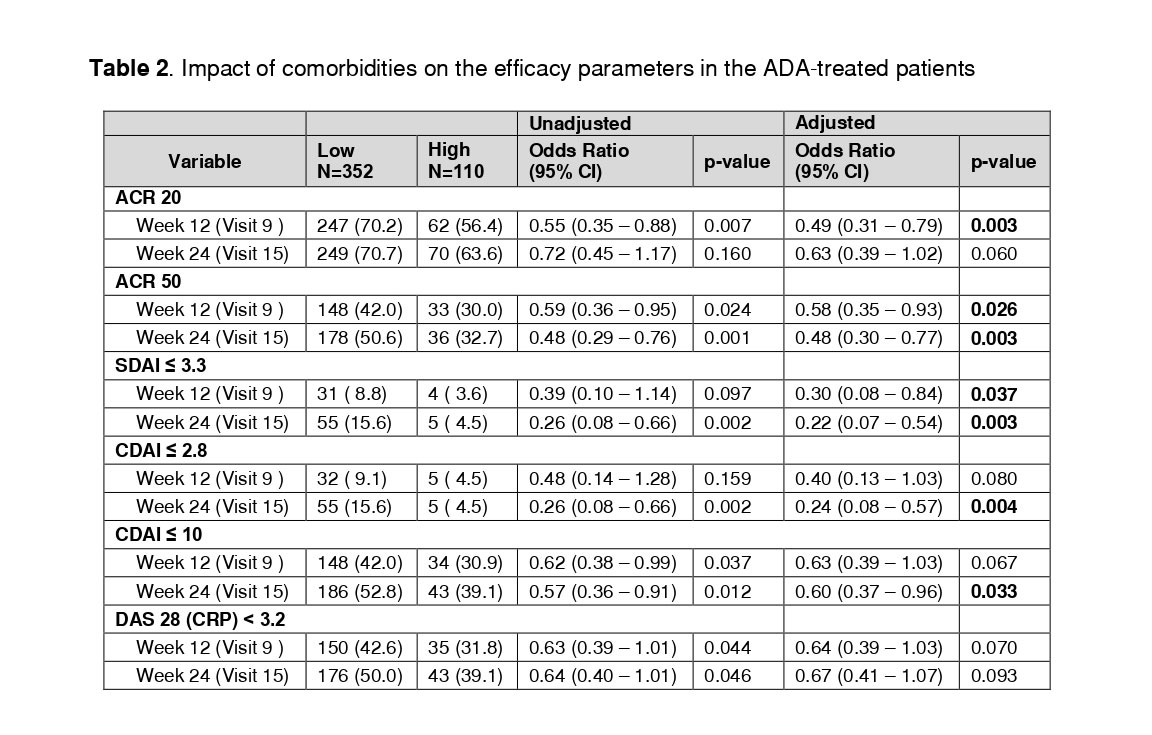
The presence of comorbid conditions affected the efficacy of ADA therapy. In the group of High CCI, the proportions of patients who achieved ACR 20 response at Week 12, ACR 50 response (Weeks 12 and 24), SDAI ≤ 3.3 (Weeks 12 and 24), CDAI ≤ 2.8 (Week 24) and CDAI ≤ 10 (Week 24) were significantly lower in comparison with the group of Low CCI (Table 2).
Conclusion: In general, there are no differences in efficacy parameters between the groups of RA patients with High and Low comorbidity burden treated with OKZ. In the group of RA patients treated with ADA, presence of at least one additional comorbid condition (high CCI) was associated with significantly lower treatment efficacy.
To cite this abstract in AMA style:
Nasonov E, Feist E, Luggen M, Yakushin S, Bukhanova D, Egorova A, Grishin S, Samsonov M, Smolen J. The Impact of Comorbidities on the Efficacy of IL-6 Inhibitor Olokizumab Compared to Adalimumab [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/the-impact-of-comorbidities-on-the-efficacy-of-il-6-inhibitor-olokizumab-compared-to-adalimumab/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-impact-of-comorbidities-on-the-efficacy-of-il-6-inhibitor-olokizumab-compared-to-adalimumab/