Session Information
Date: Monday, November 8, 2021
Title: Health Services Research Poster II: Care Models and Innovation (1061–1082)
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: Patients with SLE are disproportionately from populations with lower socioeconomic status and poorer access to health care, placing them at risk for potentially avoidable acute care use (emergency department [ED] visits and hospitalizations that could be avoided if high-quality outpatient care were provided). We defined potentially avoidable acute care conditions using the Agency for Healthcare Research and Quality’s 10 prevention quality indicators for adults and a recently published set of 25 SLE-specific, ambulatory care-sensitive outcomes1 (Table 1). A nurse-led, primary care-based integrated care management program (iCMP) at our multihospital system coordinates care for patients at high-risk for frequent acute care use due to comorbidities, demographics, and prior use patterns. We studied whether iCMP was effective at decreasing rates of potentially avoidable ED visits and hospitalizations among patients with SLE.
Methods:
We identified adults with SLE enrolled in iCMP from January 2012-February 2019. We then used electronic health record (EHR) data linked to insurance claims to compare incidence rates of potentially avoidable ED visits (composite variable and individual conditions) and potentially avoidable hospitalizations (composite variable and individual conditions) during iCMP enrollment vs. during the 12-months prior to iCMP enrollment. We used Poisson regression to compare incidence rate ratios (IRR) during iCMP versus pre-iCMP for each utilization measure, adjusted for age, sex, race/ethnicity, number of comorbidities, and calendar year, accounting for within-patient clustering. All upper gastrointestinal (GI) bleeds and osteoporotic fractures were considered potentially avoidable as we did not have information about whether patients were taking GI protectants or osteoporosis therapy.
Results: We identified 67 iCMP enrollees with SLE and linked EHR-claims data. Sixty-one of 67 met 1997 ACR criteria for SLE; 4 met 2012 SLICC criteria and 2 did not meet criteria but were diagnosed by a rheumatologist. The mean age was 60 years; 93% were female, 55% were white, 25% Black, 16% other race, and 3% Asian; 21% were Latinx. Median iCMP enrollment time was 33 months. During iCMP enrollment, there was a decrease in the overall rate of potentially avoidable ED visits (IRR 0.50; 95% CI 0.28-0.88; see Table 2) and potentially avoidable hospitalizations (IRR 0.37; 95% CI 0.21-0.65; see Table 3). We also found that during iCMP enrollment, there was an increase in the rate of ED visits for upper GI bleed (IRR 1.28; 95% CI 1.15-1.42).
Conclusion: We found that a nurse-led, primary care-based integrated care management program is effective at decreasing the rate of potentially avoidable ED visits and hospitalizations among high-risk SLE patients. We hypothesize that this is due to optimization of outpatient care. ED visits for upper GI bleeds also increased during iCMP, possibly due to medication use (for example, steroids). Further multicenter studies of integrated care management programs are needed to confirm these findings.
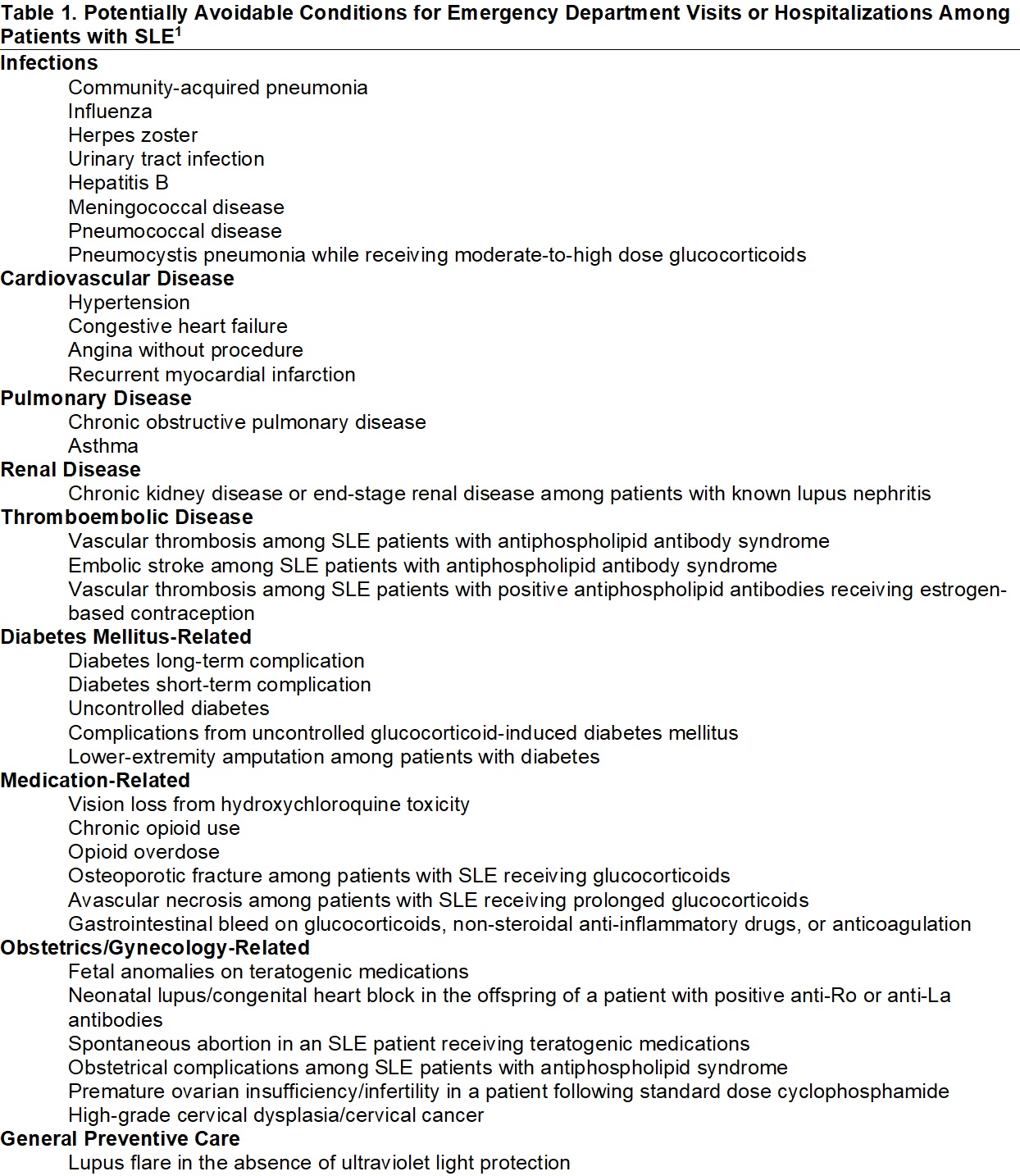 SLE=systemic lupus erythematosus 1. Feldman CH et al. Development of a Set of Lupus-Specific, Ambulatory Care-Sensitive, Potentially Preventable Adverse Conditions: A Delphi Consensus Study. Arthritis Care Res (Hoboken). 2021; 73: 146-57.
SLE=systemic lupus erythematosus 1. Feldman CH et al. Development of a Set of Lupus-Specific, Ambulatory Care-Sensitive, Potentially Preventable Adverse Conditions: A Delphi Consensus Study. Arthritis Care Res (Hoboken). 2021; 73: 146-57.
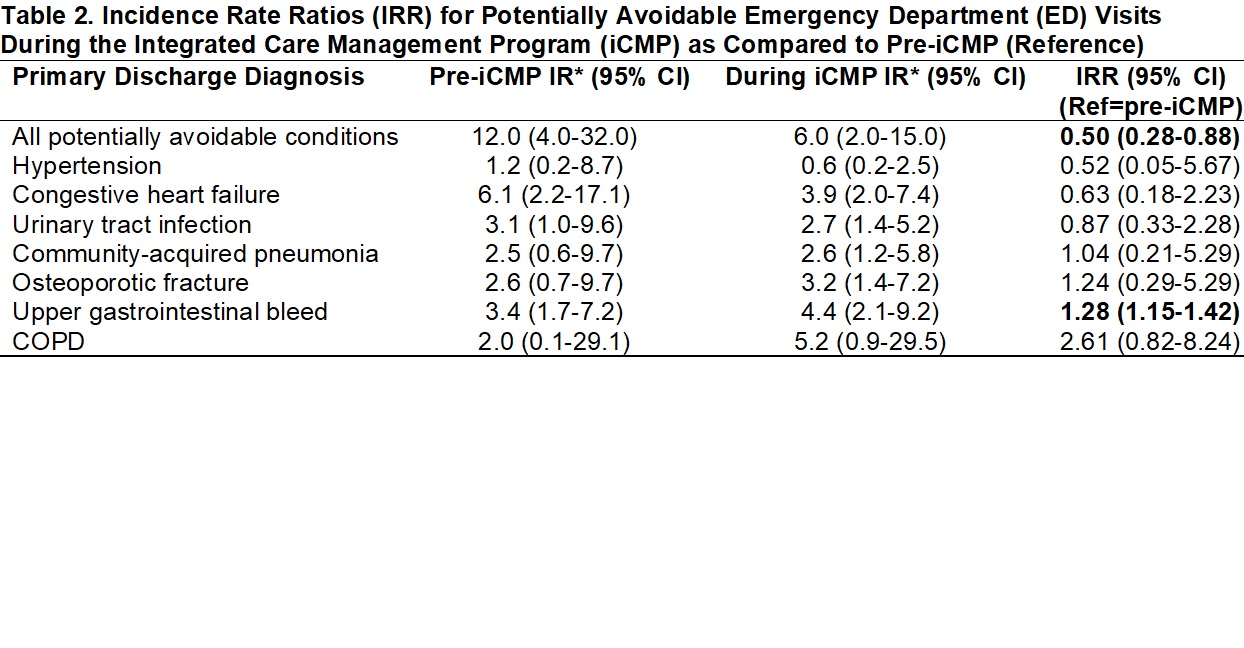 *IR per 1000 person-years; IR=incidence rate; CI=confidence interval; Ref=reference; COPD=chronic obstructive pulmonary disease; all primary discharge diagnoses which were present in our data are presented above.
*IR per 1000 person-years; IR=incidence rate; CI=confidence interval; Ref=reference; COPD=chronic obstructive pulmonary disease; all primary discharge diagnoses which were present in our data are presented above.
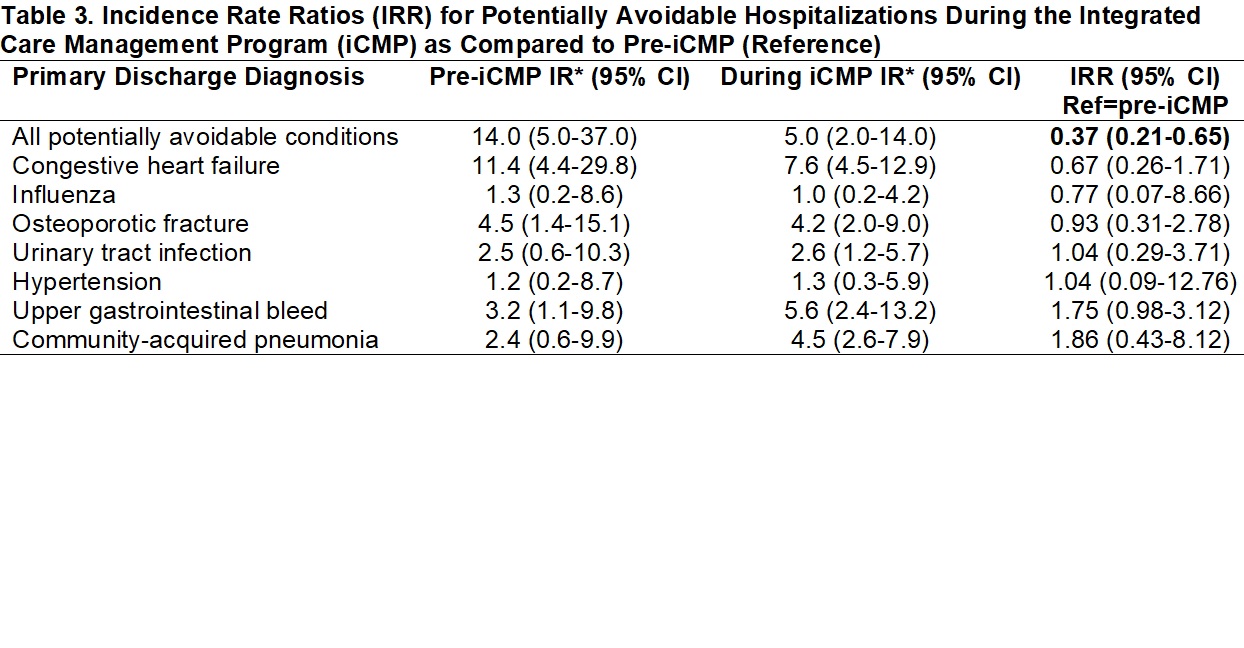 *IR per 1000 person-years; IR=incidence rate; CI=confidence interval; Ref=reference; all primary discharge diagnoses which were present in our data are presented above.
*IR per 1000 person-years; IR=incidence rate; CI=confidence interval; Ref=reference; all primary discharge diagnoses which were present in our data are presented above.
To cite this abstract in AMA style:
Williams J, Taber K, Huang W, Collins J, Cunningham R, Concannon K, Vogeli C, Wichmann L, Feldman C. The Impact of an Integrated Care Management Program on Acute Care Use for Potentially Avoidable Conditions Among High-Risk Patients with SLE [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/the-impact-of-an-integrated-care-management-program-on-acute-care-use-for-potentially-avoidable-conditions-among-high-risk-patients-with-sle/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-impact-of-an-integrated-care-management-program-on-acute-care-use-for-potentially-avoidable-conditions-among-high-risk-patients-with-sle/