Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Calcinosis is a disabling, rarely discussed manifestation of SSc for which the natural history and management is poorly understood. Last year, the Scleroderma Clinical Trials Consortium (SCTC) established a task force to develop a calcinosis specific patient reported measure (PROM). This investigation is the 1st phase of a multi-tiered project.
Methods: Four focus groups and individual interviews in the US and UK were recorded and transcribed verbatim. To capture both pathophysiologic and life impact, 2 questions were asked: 1. Since developing calcinosis how has your life changed over time? 2. How has the calcinosis changed over time? Patients were also asked to frame questions to help a physician learn if calcinosis was better, worse or the same.
Transcripts each underwent an iterative inductive process (no preconceived coding, content drives coding and analysis) by at least 5 independent analysts including at least one research team member with SSc. Concepts were triangulated to identify a comprehensive set of meaningful concepts with occurrence quantified per participant.
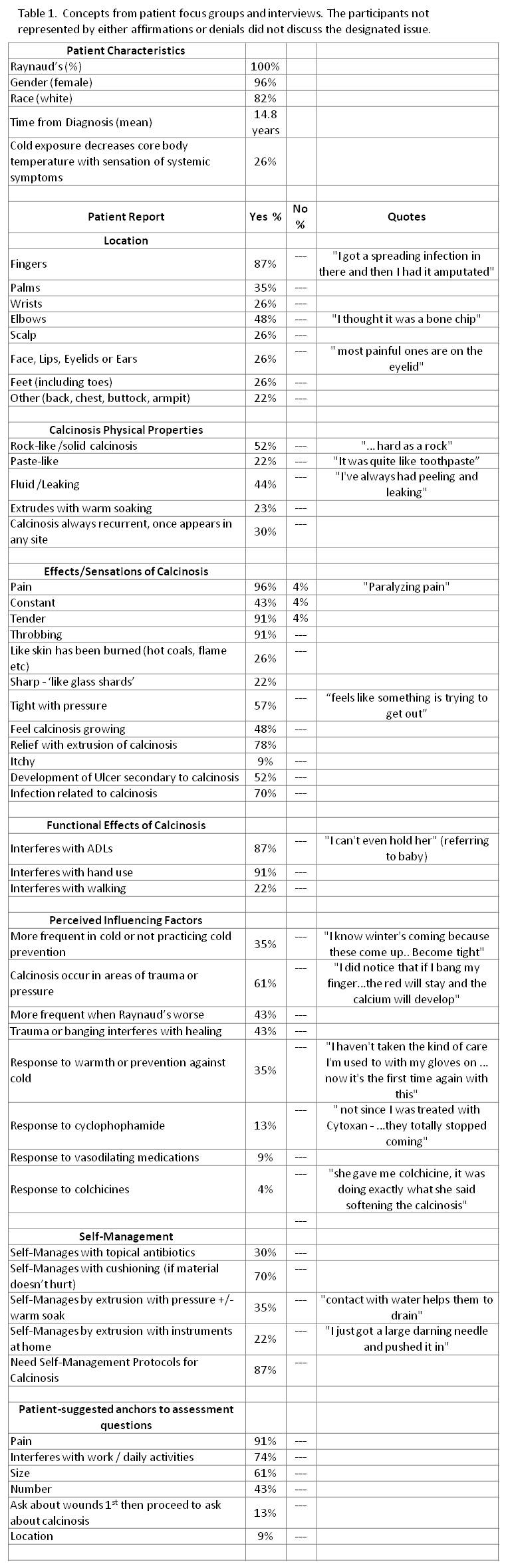
Results: Twenty-three patients (22/23 female, 19/23 white, with mean disease duration 14.8 years) were consented and interviewed. Responses spanned broadly to include concepts of self-management strategies and recurrent hypotheses relating calcinosis development to trauma, Raynaud’s and cold exposure. We identified discrete concepts which are described in Table 1 along with the proportion of patients declaring personal relevance.
Cold exposure and Raynaud’s were a perceived association to calcinosis severity – “when they are cold mine always open back up”. Several described a disabling core body phenomenon involving decreased core temperature with a rapid physical decline requiring prolonged recovery potentially lasting hours – “it’s like intense – it racks your whole body”. Calcinosis tended to present along with or soon after SSc diagnosis and remained throughout disease duration.
A majority of patients engage in strategies to extrude calcinosis with either pressure +/- soaking or at home surgical techniques. “I actually have homemade surgical tools to get these out.”
The following anchors were consistently indicated to assess calcinosis severity: pain level, size, frequency, number and functional impairment.
Conclusion: Patient observations and self-management behavior provide opportunities to learn from and to preemptively educate physicians and patients. Patients are eager for self-management guidance. These concepts provide the groundwork for PROM development. However, as suggested by patients, a composite of scales anchored in pain, size, frequency, number and related impairment may reasonably serve as an interim instrument for SSc calcinosis until that time.
Disclosure:
A. Christensen,
None;
S. Khalique,
None;
S. Cenac,
None;
K. Fligelstone,
None;
A. Mawdsley,
None;
T. Frech,
None;
J. K. Gordon,
None;
M. Baron,
None;
E. Busman,
None;
V. D. Steen,
Actelion Pharmaceuticals US,
8,
United Therapeutics,
5,
Gilead Science,
8,
Roche Pharmaceuticals,
2,
Sanofi-Aventis Pharmaceutical,
2,
CSL Berhing,
2,
Intermune,
2,
Bayer,
5;
L. A. Saketkoo,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/systemic-sclerosis-related-calcinosis-patients-provide-what-specialists-want-to-learn/