Session Information
Date: Monday, October 27, 2025
Title: (1467–1516) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients (pts) with systemic lupus erythematosus (SLE) have a significantly increased risk of atherosclerotic cardiovascular disease (ASCVD). EULAR recommends a comprehensive assessment and management of cardiovascular risk (CVR), following general population guidelines (Drosos GC et al, Ann Rheum Dis 2022). Statin therapy plays a key role in reducing CVR and preventing ASCVD events (Yousef Yengej FA et al, Neth J Med 2017). This study aimed to determine the proportion of pts with SLE eligible for statin use for primary ASCVD prevention, based on American and European CVR guidelines.
Methods: This was an observational and cross-sectional study of GLADEL 2.0, a multi-ethnic Latin-American SLE cohort. Demographics, comorbidities, medications, disease activity, and laboratory data were analyzed. Statin eligibility was determined using the 2019 American College of Cardiology/American Heart Association (ACC/AHA) and the 2021 European Society of Cardiology (ESC) guidelines. CVR was assessed using the ASCVD risk calculator from the ACC/AHA, Systemic Coronary Risk Evaluation 2 (SCORE2), and Pan American Health Organization (PAHO) risk scores. Cohen’s Kappa coefficient was used to determine inter-guideline agreement. Both guidelines only consider pts ≥40 years of age as candidates for CVR prevention with statins, due to eligibility dependence on CVR scores. Therefore, a comparative analysis was conducted between pts above and below this age threshold.
Results: Among 1083 pts in the GLADEL 2.0 SLE cohort, only 394 (36.4%) were older than 40 years of age; demographic characteristics are shown in Table 1. ACC/AHA could only be calculated for 164 pts, PAHO for 351 pts, and SCORE2 for 181 pts. Most of these pts were categorized as having a low CVR, regardless of the calculator used. A total of 15 pts were indicated to receive statin therapy based on European guidelines; among these, only 5 (33%) had a previous prescription for a statin. Among 50 pts eligible for statin therapy based on American guidelines, only 13 (26%) had been prescribed them. Inter-guideline agreement on statin eligibility was fair (Cohen’s Kappa = 0.35; 95% CI: 0.15–0.55). Pts under 40 years of age were more obese and had higher disease activity compared with those older than 40 years of age (Table 2).
Conclusion: This study reveals a gap in the management of CVR among pts with SLE in the GLADEL 2.0 cohort, as only a small percentage are candidates for statin therapy, primarily due to the predominance of younger pts under age 40. Traditional CVR assessment tools fail to encompass this group, which is at an elevated risk for accelerated atherosclerosis. Among eligible pts, statin prescribing rates remain low, suggesting a missed opportunity in proactive cardiovascular prevention. The moderate agreement between differing guidelines highlights the inconsistency in risk assessment and management approaches for this population. There is a need for tailored strategies to comprehensively evaluate and address CVR in younger pts with chronic inflammatory conditions like SLE. Implementing more inclusive guidelines could enhance preventative measures and improve outcomes for pts at increased risk for ASCVD.
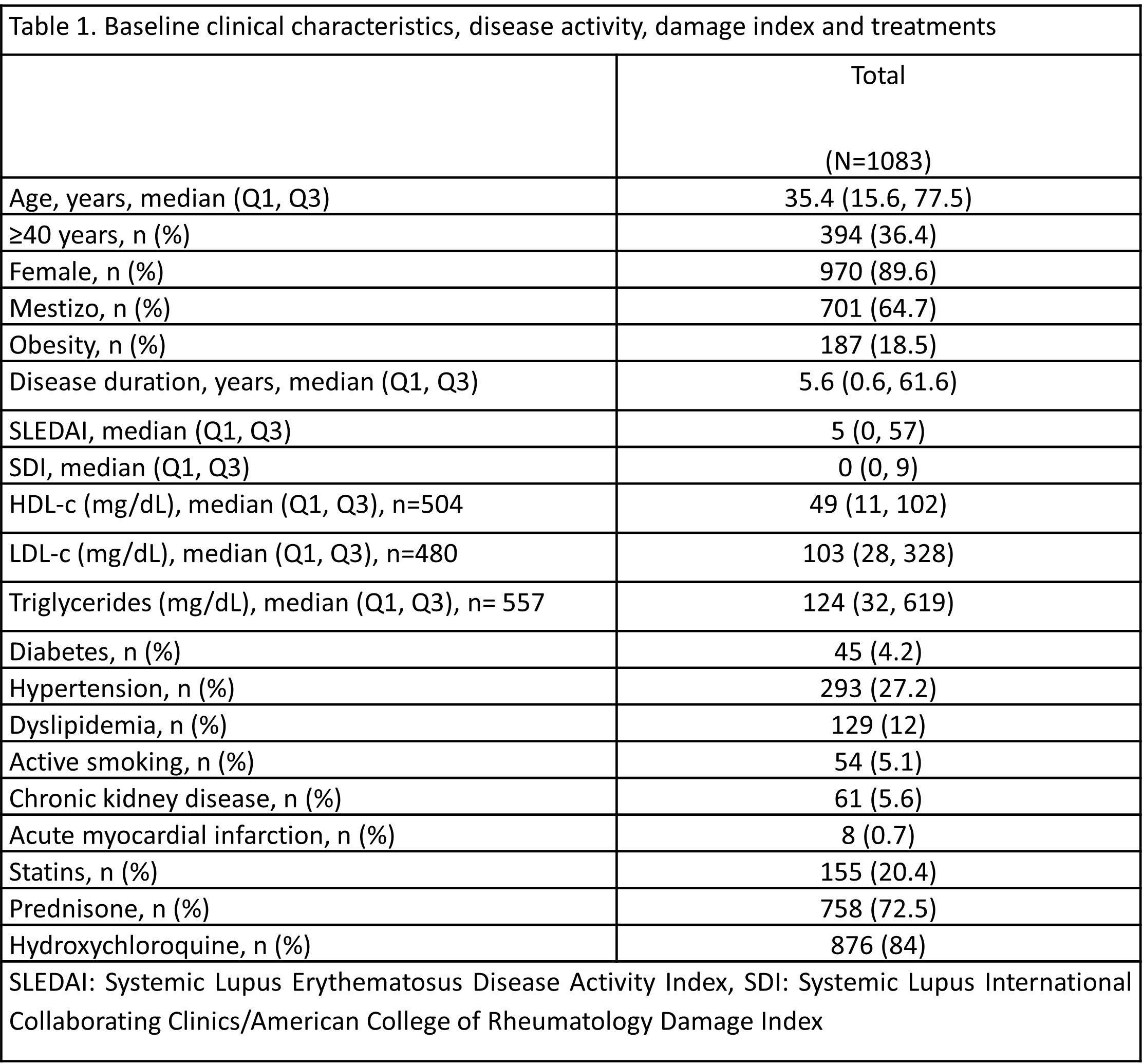 Table 1: Baseline clinical characteristics, disease activity, damage index and treatments
Table 1: Baseline clinical characteristics, disease activity, damage index and treatments
.jpg) Table 2. Comparison of clinical characteristics based on their age group.
Table 2. Comparison of clinical characteristics based on their age group.
To cite this abstract in AMA style:
Reynosa-Silva I, Colunga-Pedraza I, Harvey G, Galarza-Delgado D, Azpiri-Lopez J, Garcia-Garcia F, Garza-Flores O, Scolnik M, Subils G, OTADUY C, Saurit V, Arturi V, Berbotto L, Pons-Estel G, Lucero L, Serna Góngora M, Gargiulo M, Pisoni C, Crespo M, Guamán M, Barbosa V, Gasparin A, Mariz H, Ribeiro F, Borba E, dos Reis-Neto E, Guerra Herrera I, Massardo M, Aroca Martínez G, Cañas C, Quintana-Lopez G, Toro-Gutierrez C, Moreno Alvarez M, SAAVEDRA M, Portela Hernández M, Fragoso-Loyo H, Amezcua-Guerra L, García-De la Torre I, Velasco Santos J, Esquivel Valerio J, Losanto J, Alva Linares M, Ugarte-Gil M, Zuñiga Corrales K, Muñoz-Louis R, Pizzarossa C, Silveira G, Zazzetti F, Orillion A, Vásquez G. Systemic Lupus Erythematosus and Statins in GLADEL 2.0: Are Cardiovascular Risk Prevention Guidelines Being Followed? [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/systemic-lupus-erythematosus-and-statins-in-gladel-2-0-are-cardiovascular-risk-prevention-guidelines-being-followed/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/systemic-lupus-erythematosus-and-statins-in-gladel-2-0-are-cardiovascular-risk-prevention-guidelines-being-followed/