Session Information
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Osteoarthritis (OA) is a leading cause of disability globally, and its disease burden is expected to increase as risk factors such as aging and obesity also rise (Wallace, IJ et al. PNAS 2017). Unmet needs remain for safe and efficacious treatments for both symptoms and structural modification. Disease heterogeneity and the difficulties assessing pain and joint structure in clinical trials are challenges to developing effective treatments options. This post hoc analysis of lorecivivint (LOR), an intra-articular (IA) CLK/DYRK inhibitor that modulates Wnt and inflammatory pathways, examined the structural heterogeneity of participants enrolled in Phase 2 and 3 LOR trials and then the associated treatment responses within KL grade subgroups. The purpose of this analysis was to identify potential relationships between OA pain and knee joint structure which may aid future clinical trial design.
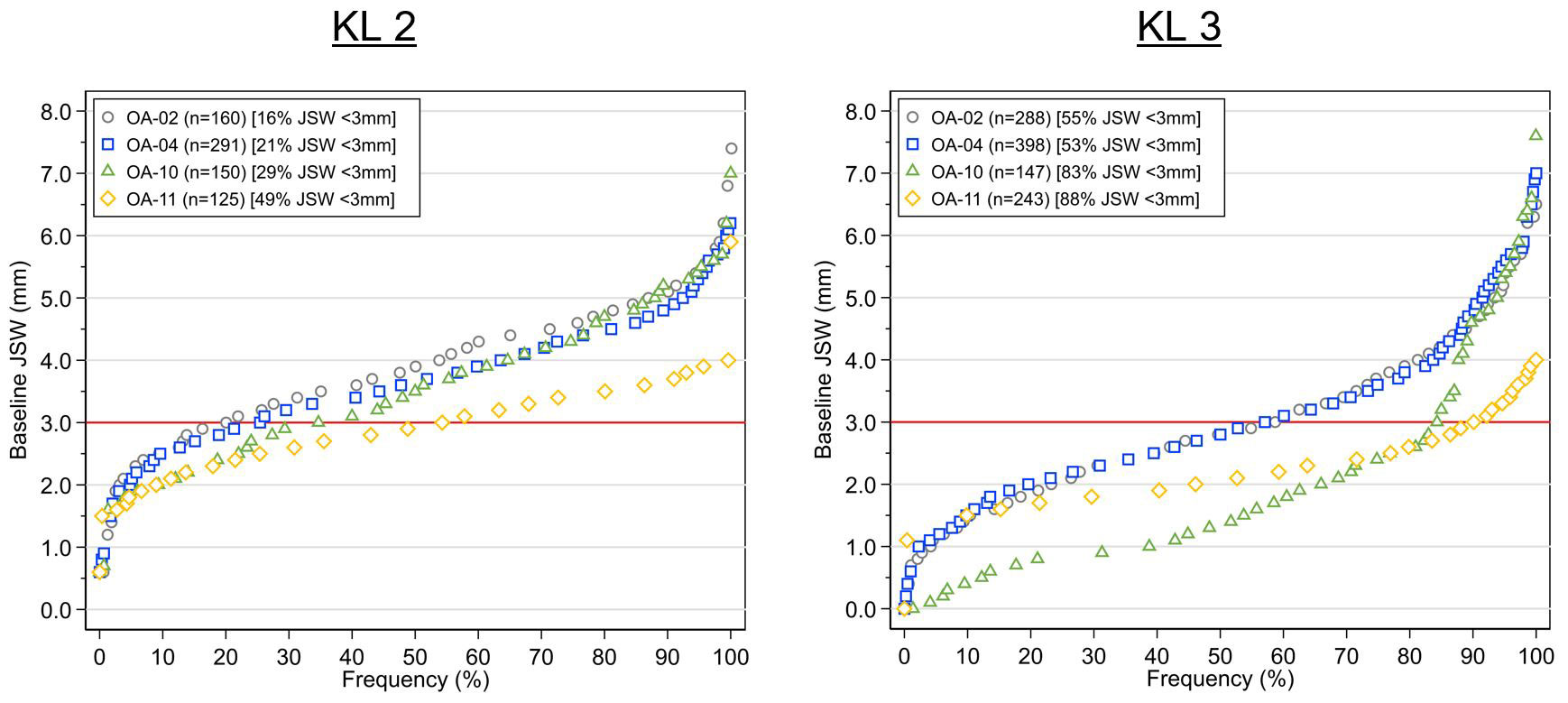
Methods: Data was analyzed from two Phase 2 (OA-02, NCT02536833; OA-04, NCT03122860), and two Phase 3 trials (OA-10, NCT04385303; OA-11, NCT03928184). In all trials, participants had ACR-defined (clinical and radiographic) knee OA, Kellgren-Lawrence (KL) grades 2-3. For OA-04, OA-10 and OA-11, additional criteria included Pain Numeric Rating Scale (NRS) [0-10] ≥4 and ≤8 in the target knee and < 4 in the contralateral knee. Baseline JSW for each study was compared using a cumulative frequency distribution plots by KL grade; percentages of subjects with JSW < 3mm for each study was also summarized to provide a surrogate for loss of ~50% healthy JSW (Deep et al. JBJS 2003). For the trials which captured Pain NRS, treatment responses were assessed according to KL grade and by trial. For all treatment-related outcomes, change from baseline was estimated using baseline-adjusted ANCOVA at each timepoint.
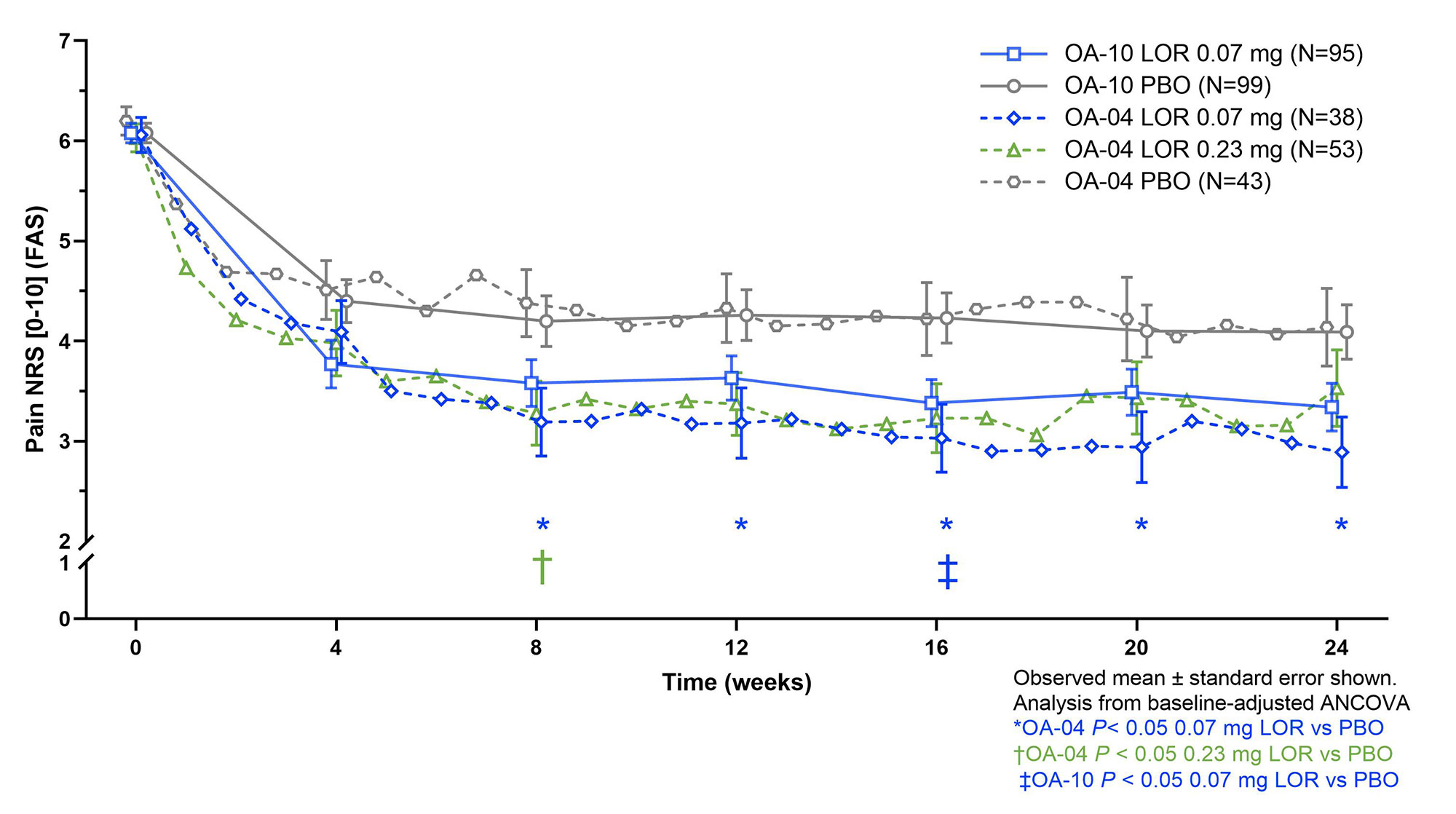
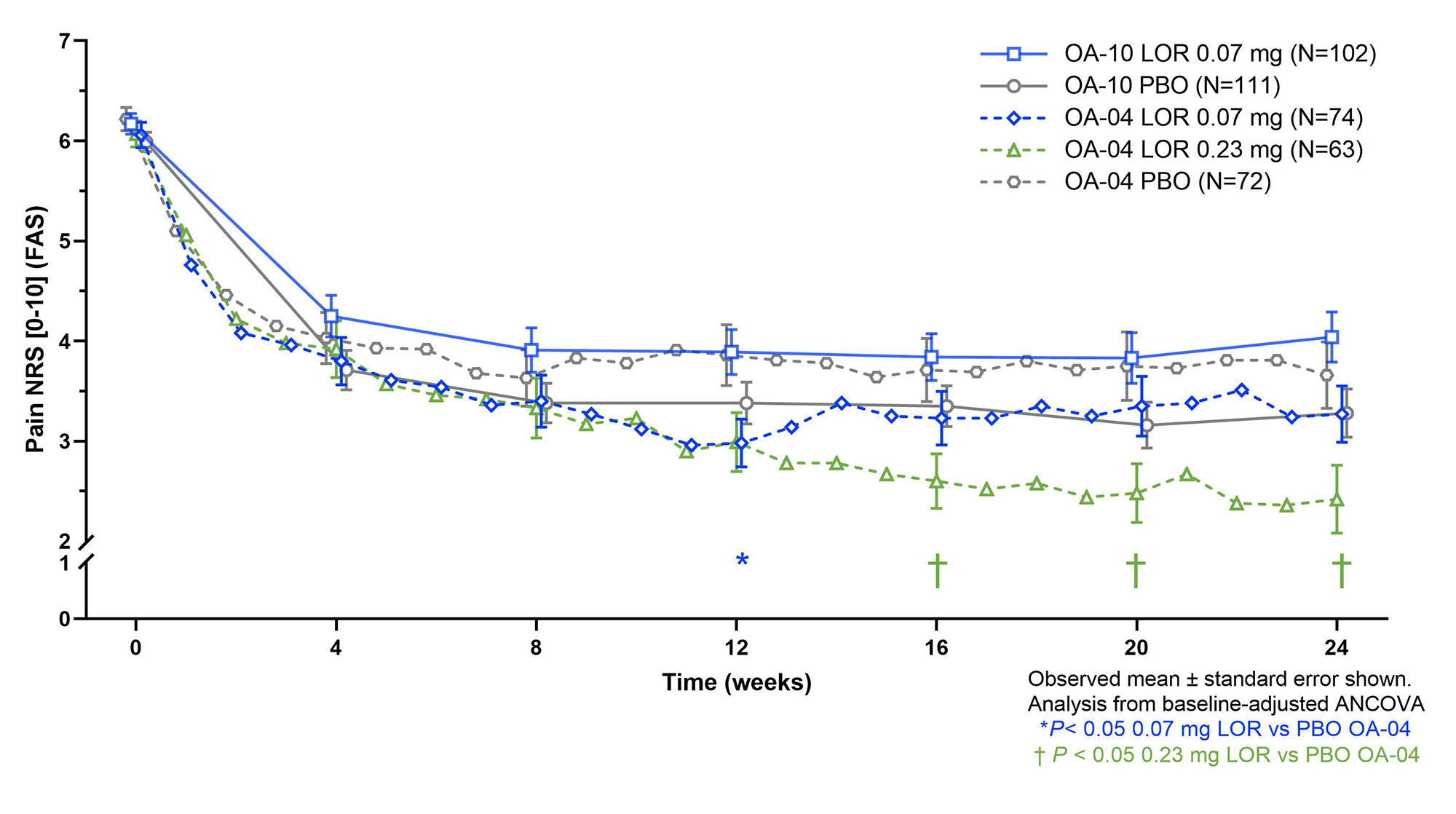
Results: In the Phase 2 trials, 16% (OA-02) and 21% (OA-04) and in the Phase 3 trials, 30% (OA-10) and 49% (OA-11) of KL 2 participants had baseline mJSW < 3 mm. For KL 3 participants, OA-02 had 55% and OA-04 53%, while OA-10 had 81% and OA-11 88% mJSW < 3mm (figure 1). Beneficial treatment effect of LOR vs. PBO was seen in KL 2 for OA-04 and OA-10, but not OA-11, with similar magnitude of response seen for 0.07 mg and 0.23 mg doses (figure 2). Beneficial treatment effect of LOR was seen only in OA-04 for KL 3, with similar magnitude of change for 0.07 mg and 0.23 mg LOR through week 12, and greater improvement observed for the 0.23 mg dose for weeks 12-24 (figure 3).
Conclusion: In this post hoc analysis, there was substantial heterogeneity in baseline mJSWs across LOR clinical trials within the KL 2-3 grade inclusion criteria. Participants with less structurally advanced knee OA showed greater pain treatment responses to 0.07 mg LOR compared to those with more advanced disease. These data support the hypothesis that the amount of OA structural damage is associated with the pain of knee OA and that earlier intervention may improve outcomes.
To cite this abstract in AMA style:
Yazici Y, Swearingen C, Ghandehari H, simsek i, Kennedy S, Tambiah J, McAlindon T. Structural Severity in Knee Osteoarthritis Impacts Treatment Response: A Post Hoc Pooled Analysis of Lorecivivint Clinical Trials [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/structural-severity-in-knee-osteoarthritis-impacts-treatment-response-a-post-hoc-pooled-analysis-of-lorecivivint-clinical-trials/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/structural-severity-in-knee-osteoarthritis-impacts-treatment-response-a-post-hoc-pooled-analysis-of-lorecivivint-clinical-trials/