Session Information
Date: Friday, November 6, 2020
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster I: Clinical Manifestations
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Clinical trials and observational studies in lupus nephritis (LN) have shown that proteinuria level at 12 months is the best predictor of long-term renal outcomes (adequate renal function and no dialysis/ transplant), although proteinuria can be a slowly changing parameter with a recovery time often beyond 2 years. Given the high morbidity of LN, an accessible, rapidly responsive biomarker may serve as a useful adjunct to proteinuria in assessing early treatment response.
The aim of this study was to determine if serum albumin can serve as predictor of complete (CPR) and partial proteinuria recovery (PPR) at 6-9 and 18-21 months in LN patients receiving standard treatment.
Methods: We studied all patients followed at the Lupus Clinic from 1990 onwards with baseline and follow-up visits at 6-9 and 18-21 months. Patients were diagnosed with LN based on 24-hour urine proteinuria > 0.5 g/24 hours or a spot urinary protein/creatinine ratio (UPCR) > 0.5 g/g associated with a prednisone start of ≥ 10 mg or a dose escalation of ≥ 5 mg.
CPR was defined as UPCR < 0. 5 g/g. PPR was defined as UPCR < 1.0 g/g (if baseline ≤ 3.0 g/g) or UPCR ≤ 3.0 g/g (if baseline PCR > 3.0 g/g) as defined by Rovin [LUNAR] criteria. We compared this to SLE Disease Activity Index-2000 (SLEDAI-2K) which defines CPR as proteinuria < 0.5g/24 hours and the SLEDAI-2K Responder Index-50 (SLEDAI-2K RI50) which defines PPR as a ≥ 50% decrease in proteinuria from baseline. Complete recovery of serum albumin was defined as ≥ 35 g/L from a baseline of < 30 g/L, with partial recovery defined as ≥ 30 g/L but < 35 g/L from a baseline of < 30 g/L.
Receiver operating characteristic (ROC) curves were generated to test if serum albumin is a predictor of combined proteinuria recovery endpoint (PPR+CPR as defined by Rovin criteria) at 6-9 and 18-21 months. Area under curve (AUC) was analyzed for (a) albumin level at baseline (b) absolute change from baseline to 6-9 and 18-21 months, and (c) percent change between baseline to 6-9 and 18-21 months.
Results: 161 patients with 6-9 month visits (83.9% female) were identified. The mean age and duration of lupus at the start of the study was 34.7 ± 12.6 and 5.2 ± 5.6 years.
At the 6-9 month visit, 22% of patients achieved PPR and 42% of patients achieved CPR (64% combined). Of the 161 patients, 31 (19.3%) had a baseline albumin < 30 g/L. Of the 94 patients with an 18-21 month visit, 17% achieved PPR and 54% achieved CPR (71% combined). Both Rovin and SLEDAI-2K RI-50 criteria identified similar percentage of responders.
ROC curves showed serum albumin absolute change (AUC= 0.75) and percent change (AUC=0.75) from baseline to 6-9 months predicted 6-9 month proteinuria recovery. Similarly, serum albumin absolute change (AUC= 0.78) and percent change (AUC=0.78) from baseline to 18-21 months predicted proteinuria recovery at 18-21 months. Serum albumin levels at baseline were not predictive of proteinuria recovery at 6-9 months or 18-21 months (AUC 0.54).
Conclusion: Absolute and percent change in serum albumin from baseline to 6-9 and to 18-21 months is a good predictor of proteinuria recovery. Serum albumin may serve as a readily accessible adjunct to proteinuria in assessing clinical course and treatment response in LN.
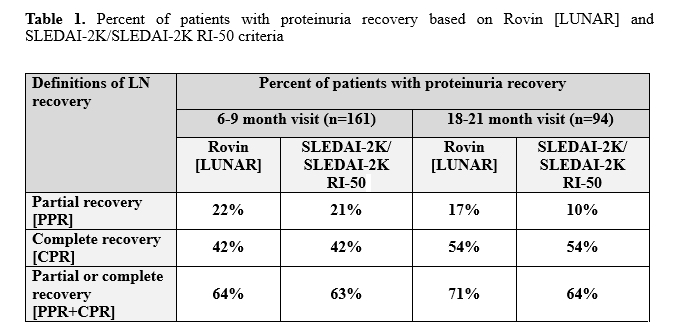 Table 1. Percent of patients with proteinuria recovery based on Rovin [LUNAR] and SLEDAI-2K/SLEDAI-2K RI-50 criteria
Table 1. Percent of patients with proteinuria recovery based on Rovin [LUNAR] and SLEDAI-2K/SLEDAI-2K RI-50 criteria
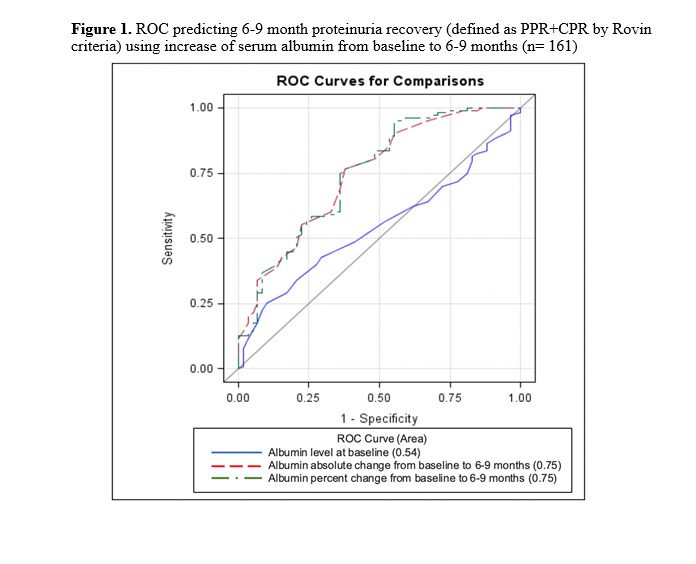 Figure 1. ROC predicting 6-9 month proteinuria recovery (defined as PPR+CPR by Rovin criteria) using increase of serum albumin from baseline to 6-9 months (n= 161)
Figure 1. ROC predicting 6-9 month proteinuria recovery (defined as PPR+CPR by Rovin criteria) using increase of serum albumin from baseline to 6-9 months (n= 161)
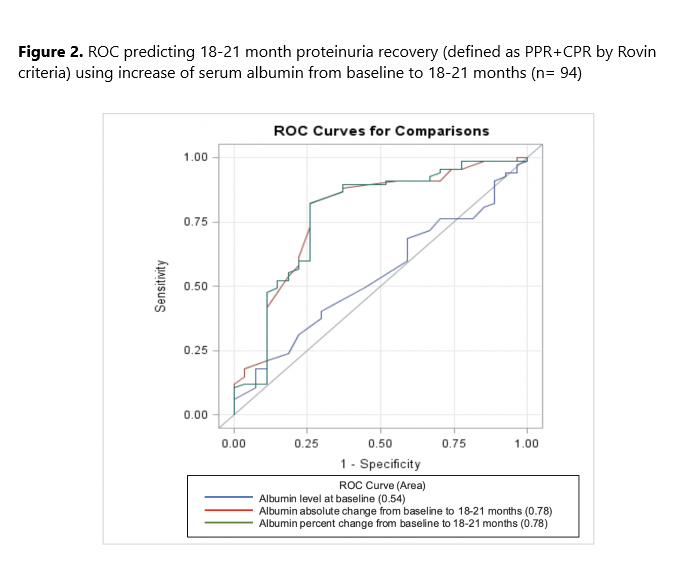 Figure 2. ROC predicting 18-21 month proteinuria recovery (defined as PPR+CPR by Rovin criteria) using increase of serum albumin from baseline to 18-21 months (n= 94)
Figure 2. ROC predicting 18-21 month proteinuria recovery (defined as PPR+CPR by Rovin criteria) using increase of serum albumin from baseline to 18-21 months (n= 94)
To cite this abstract in AMA style:
Tofighi T, Reich H, Su J, Touma Z. Serum Albumin as a Predictor of Proteinuria Recovery in Lupus Nephritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/serum-albumin-as-a-predictor-of-proteinuria-recovery-in-lupus-nephritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/serum-albumin-as-a-predictor-of-proteinuria-recovery-in-lupus-nephritis/