Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Scleroderma heart involvement (SHI) is the 3rd leading cause of death in systemic sclerosis (SSc) [1] following interstitial lung disease (ILD) & pulmonary arterial hypertension (PAH). There are specific guidelines to diagnose & effectively manage ILD & PAH, but SHI remains poorly understood and underdiagnosed due to lack of unified definition or acceptable diagnostic testing. Its prevalence and risk factors are unknown.
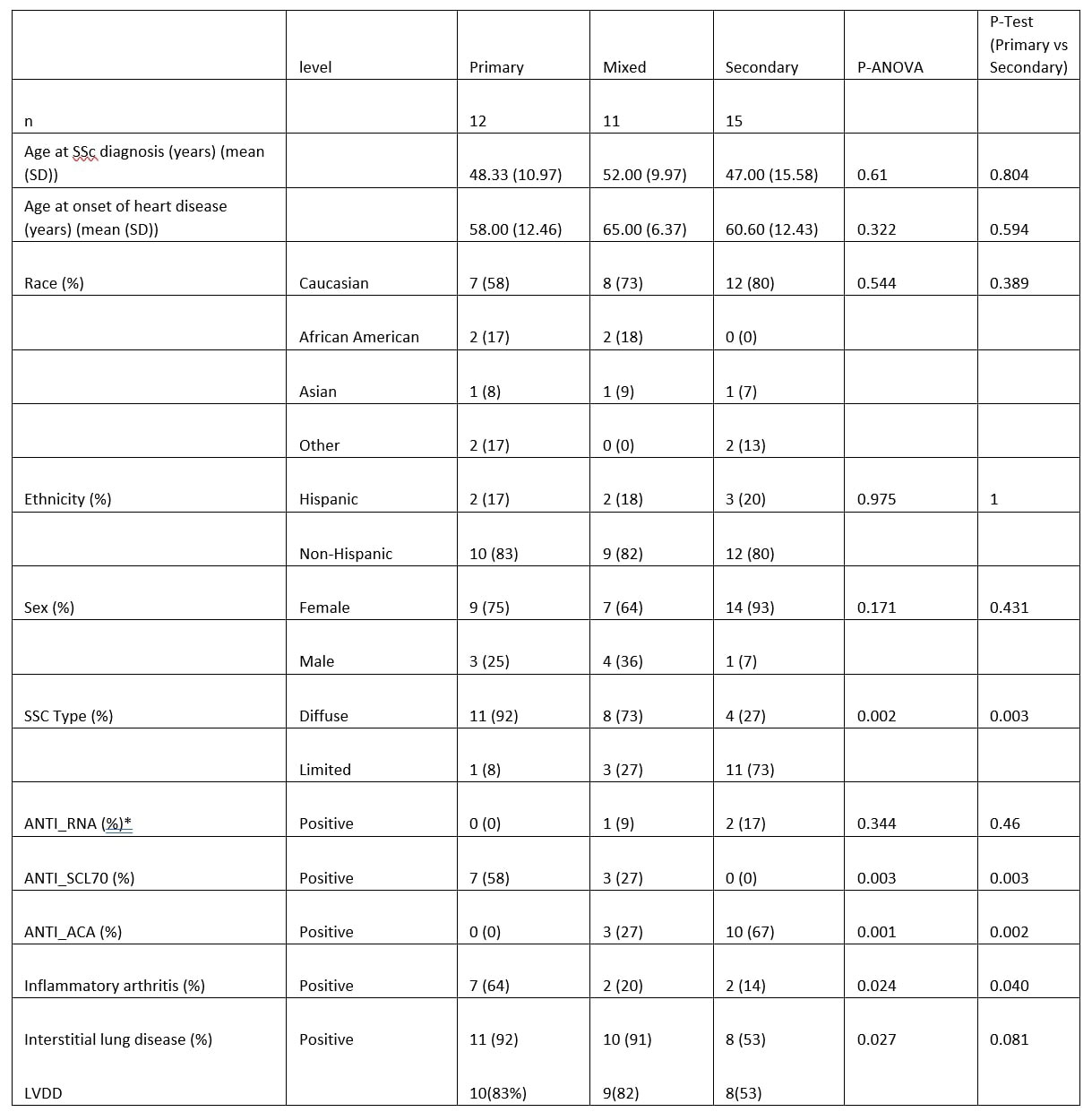
Methods: Upon IRB approval, we reviewed electronic medical records of 38 randomly selected SSc subjects with heart disease from various causes, from our outpatient Scleroderma Program. They fulfilled the 2013 ACR/EULAR classification criteria [4] for SSc and their cardiac disease was obtained from past or present history & corroborated by abnormal imaging, including Echo/Doppler, cardiac MRI, EKG, Holter monitor, stress test, or myocardial biopsy, or other miscellaneous tests to identify cardiac disease manifestations. We collaborated with an expert cardiologist to define the following 3 groups of cardiac disease: 1) likely due to primary SHI (or cardiac abnormalities, directly attributed to scleroderma), 2) Secondary heart disease if their heart disease could be readily explained by another cause unrelated to scleroderma, or 3) mixed etiologies.
Results: There were 12 patients with primary SHI, 11 patients with mixed & 15 with secondary causes of their heart disease. Those with primary SHI were significantly associated with presence of diffuse cutaneous scleroderma (p=0.03), inflammatory arthritis (p=0.04), and the ScL70 antibodies (p = 0.03). Subjects with ACA antibodies were significantly protected from developing primary SHI (p = 0.002). Nearly all of those with primary SHI had ILD, compared to about half of those with secondary SHI (92% vs. 53%, p=0.081). 83% of patients with primary SHI had LVDD, 82% of patients with mixed heart disease had LVDD compared to 53% of patients with secondary heart disease had LVDD. This was not statistically significant.
Conclusion: SHI remains poorly understood & under-diagnosed due to its diverse & often subclinical presentation. Our small cohort found subjects with diffuse SSc, Scl70 antibody, presence of inflammatory arthritis and ILD as risk factors associated with having primary SHI. Larger studies are sorely needed to identify & better manage our patients with primary SHI.
To cite this abstract in AMA style:
Talaat M, Hsu V, Shindler D. Scleroderma Heart Disease [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/scleroderma-heart-disease/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/scleroderma-heart-disease/