Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Treatment with rituximab (RTX) has presented a challenge during the COVID-19 pandemic, as antibody response after primary vaccination are markedly reduced and often undetectable.The primary outcome of this study was to investigate the percentage of RTX treated RD patients without detectable antibody responses after two vaccinations that mounted detectable antibody responses after a booster vaccination (3rd dose) or revaccination (3rd and 4th) vaccine dose. The secondary outcome was to examine if the level of B-cells in peripheral blood predicted the antibody response.
Methods: We included 91 RD patients, who had recieved RTX within the past 24 months and were vaccinated against COVID-19 with an mRNA vaccine. Patients were offered revaccination or a single booster vaccination with an mRNA vaccine. Serum total antibodies and specific IgG against SARS-CoV-2 spike protein were measured before and six weeks after the last vaccine dose. B-cells (CD19+CD45+) were measured by flow cytometry at inclusion. Logistic regression analyses were performed with the presence of SARS-CoV-2 antibodies after vaccination as the dependent variable.
The study was supported by an urestricted grant from the The Danish Rheumatism Association.
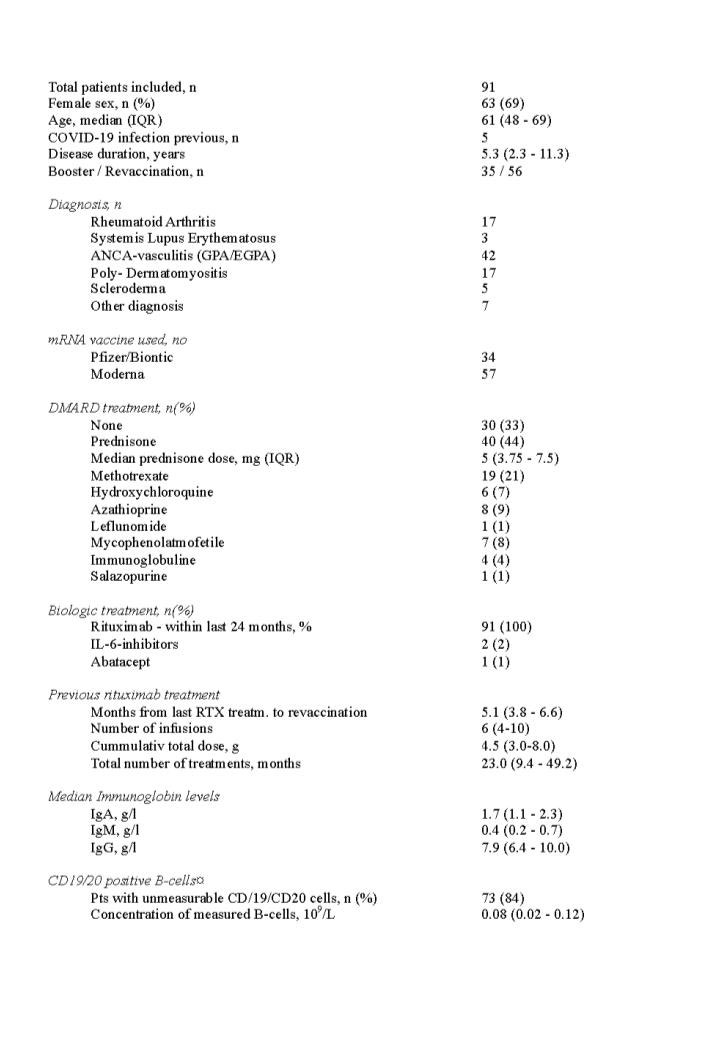
Results: Patient characteristics are given in Table 1. Most participants were female (69%) with a median age of 61 years, and the most common diagnosis were vasculitis (45%), rheumatoid arthritis (19%) and myositis (19%).
Sixty-nine patients had undetectable anti-SARS-CoV-2 antibody levels after the initial vaccination. In these patients, 5 out 13 (38%) who recieved a booster dose and 18/56 (32%) who recieved a revaccination seroconverted, Figure 1A. This difference was not significant (p=0.67). Patients receiving re-vaccination had significantly higher antibody levels than patients receiving a booster dose (p< 0.001), Figure 1A.
Nearly all patients (7/8, 87.5 %), who had quantifiable B-lymphocytes but were seronegative before re-vaccination or boosting achieved detectable SARS-CoV-2 antibodies after six weeks (Fig. 1b). In contrast, 16 out of 58 patients (27.6%) with unquantifiable B-lymphocytes and unmeasurable antibodies before vaccination developed antibodies 6 weeks after booster/revaccination.
In both univariate and multivariate logistic regression analysis, only B-cells higher than 10/µL before boost or revaccination were associated with seroconversion (p=0.009 and p=0.01, respectively), Table 2. Seroconversion was independent of age, gender, diagnosis, cumulative RTX dose, RTX treatment time, and time since last RTX treatment.
Conclusion: Continuously impaired humoral response to mRNA vaccines was found in most RTX treated RD patients after a booster dose (one-dose) or revaccination (two-doses). Re-vaccination lead to significantly higher antibody levels in patients who did not have a detecable humoral responce after the first two vaccine doses, compared to a booster dose. CD19+ B-cells are a significant predictor of humoral responce to vaccination. However, more than half of the patients with no measureable B-cells pre-vaccination developed a detecable humoral responce after revaccination.


To cite this abstract in AMA style:
Ammitzboell C, thomsen m, Andersen J, Jensen J, Hermansen m, Johannsen a, Larsen M, Mistegaard C, Mikkelsen S, Szabados F, Vils S, Erikstrup C, Hauge E, Troldborg A. Rituximab-treated Rheumatic Patients: B-cell Levels Predict Sero-conversion After COVID-19 Boost or Re-vaccination in Initial Vaccine Non-responders [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/rituximab-treated-rheumatic-patients-b-cell-levels-predict-sero-conversion-after-covid-19-boost-or-re-vaccination-in-initial-vaccine-non-responders/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rituximab-treated-rheumatic-patients-b-cell-levels-predict-sero-conversion-after-covid-19-boost-or-re-vaccination-in-initial-vaccine-non-responders/