Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: The aim of the present work is to determine the fracture risk associated with glucocorticoids requiring diseases
Methods: We conducted a retrospective analysis of a nation-wide cohort (DeFRACalc79 database). We collected many clinical variables, including the use of glucocorticoids, the presence of prior hip or vertebral and non-vertebral or non-hip fractures and the presence of comorbidities (rheumatoid arthritis, psoriatic arthritis, undifferentiated connective [UCTD], systemic lupus erythematosus [SLE], systemic sclerosis, chronic obstructive pulmonary disease [COPD], multiple sclerosis, chronic inflammatory bowel diseases [IBD], severe physical handicap, diabetes, Parkinson’s and HIV). We generated age and T-score matched groups of patients with and without comorbidities via propensity score matching. After 1:1 matching we analyzed the prevalence of fragility fractures. We performed a sensitivity analysis by eliminating all patients who used glucocorticoids ≥5 mg/day for ≥3 months.
Results: 59950 women aged 65.1 years (SD 11.0), with total-hip T-score of -2.16 (SD 0.94) and lumbar spine T-score of –2.50 (SD 1.15) were included in the analysis. Among 13,546 women with comorbidity 3114 (23.0%) had diabetes; 3008 (22.2%) rheumatoid arthritis; 1910 (14.1%) UCTD; 1614 (11,9%) BPD; 942 (7,0%) IBD; 794 (5,9%) severe motor disability; 703 (5,2%) psoriatic arthritis; 412 (3,0%) Parkinson’s. 294 (2,2%) LES; 277 (2,0%) systemic sclerosis; 243 (1,8%) multiple sclerosis and 235 (1,7%) had HIV. Figure 1 shows the prevalence of glucocorticoid use stratified by disease. Glucocorticoid intake ≥5 mg/day for ≥3 months (after 1:1 matching by age and T-scores) was significantly associated with vertebral fractures (aOR 1.5 95% CI 1.3-1.7) but not with non-femoral non-vertebral fractures (aOR 1.0 95% CI 0.9-1.2) while intake of ≥5 mg/day for ≥12 months was associated with fractures of all kind (aOR 1.3 95% CI 1.2-1.3 and 1.3 95% CI 1.1-1.8). Figure 2 and Figure 3 show the ORs for the presence of vertebral or hip fractures and non-vertebral or non-hip fractures (glucocorticoid users and non-users respectively). Diseases with increased risk of fracture, independently from glucocorticoid intake, were rheumatoid arthritis, COPD and severe physical handicap for non-vertebral and non-hip fractures and COPD and IBD for vertebral or hip fractures.
Conclusion: At a population level, glucocorticoid intake is still common, especially in patients with rheumatic diseases, and is associated with an increased risk of fractures, both vertebral, hip and non-vertebral non-hip fractures. Rheumatoid arthritis, COPD and severe physical handicap were independently associated with an increased risk of non-vertebral and non-hip fractures whereas only COPD and IBD were associated with vertebral or hip fractures.
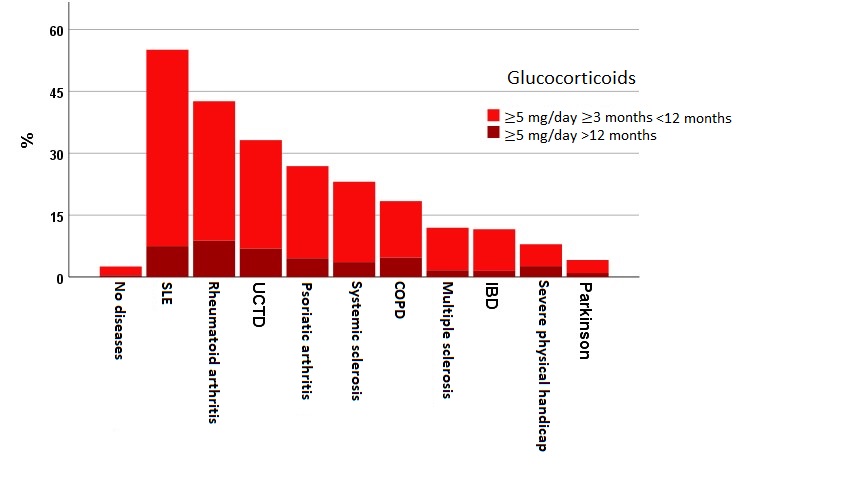 Figure 1. Glucocorticoid use in the cohort under analysis
Figure 1. Glucocorticoid use in the cohort under analysis
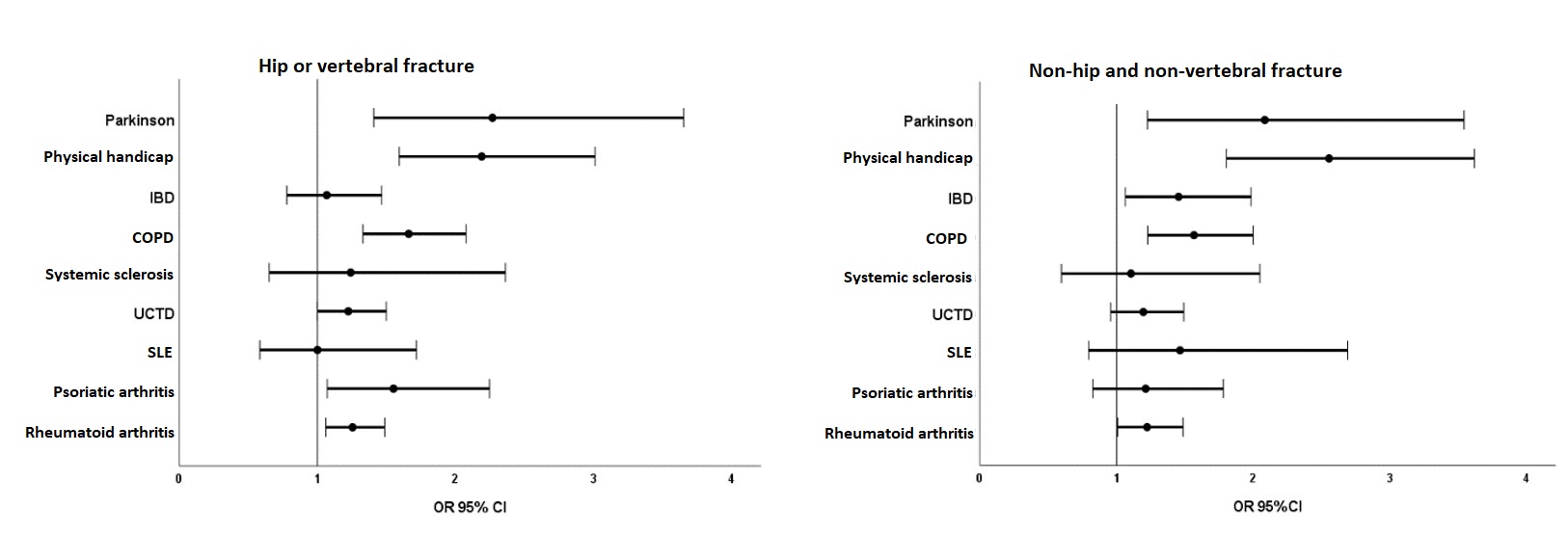 Figure 2. Odd ratios of vertebral and hip fracture and non-vertebral, non-hip fractures in the study population
Figure 2. Odd ratios of vertebral and hip fracture and non-vertebral, non-hip fractures in the study population
 Figure 3. Odd ratios of vertebral and hip fracture and non-vertebral, non-hip fractures in the study population (excluding glucocorticoid users)
Figure 3. Odd ratios of vertebral and hip fracture and non-vertebral, non-hip fractures in the study population (excluding glucocorticoid users)
To cite this abstract in AMA style:
Adami G, Fassio A, Giollo A, Idolazzi L, Viapiana O, Gatti D, Rossini M. Risk of Fracture in Patients with Different Glucocorticoid Requiring Diseases [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/risk-of-fracture-in-patients-with-different-glucocorticoid-requiring-diseases/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/risk-of-fracture-in-patients-with-different-glucocorticoid-requiring-diseases/