Session Information
Date: Sunday, November 13, 2016
Title: Osteoarthritis – Clinical Aspects I: Epidemiology and Progression
Session Type: ACR Concurrent Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Accelerated knee osteoarthritis (KOA) is a painful disorder and associated with several risk factors: greater age, greater body mass index (BMI), static knee alignment, and coronal tibial slope. While no single risk factor can accurately predict who is at risk for accelerated KOA, it would be beneficial to recognize the combinations of risk factors that identify people at risk for accelerated KOA. Hence, we assessed which combinations of risk factors can classify adults who develop accelerated KOA or not and which risk factors are most important.
Methods: We conducted a case-control study using data from baseline and the first 4 annual visits of the Osteoarthritis Initiative. Eligible participants had no radiographic KOA at baseline (Kellgren-Lawrence [KL] < 2). We classified 3 groups: 1) accelerated KOA: ≥ 1 knee progressed to advance-stage KOA (KL 3 or 4) within 48 months, 2) typical onset of KOA: ≥ 1 knee increased in radiographic scoring within 48 months (excluding those defined as accelerated KOA), and 3) No KOA: no change in KL grade by 48-months. We did 1:1:1 matching for the 3 groups based on sex. A laboratory blinded to group assignment conducted serum assays in duplicate for CRP, GSP, and glucose concentrations. Staff recorded age, sex, and BMI based on standardized protocols. Weight-bearing, fixed flexion posterior-anterior knee radiographs were obtained at baseline and follow-up visits. One reader manually measured baseline coronal tibial slope (ICC = 0.87). Baseline femorotibial alignment angle was measured on the radiographs using a semi-automated program software tool. We performed classification and regression tree (CART) analysis to determine rules for classifying individuals as accelerated KOA or not (no KOA and gradual onset) based on baseline age, BMI, coronal tibial slope, static alignment, serum measures, and sex.
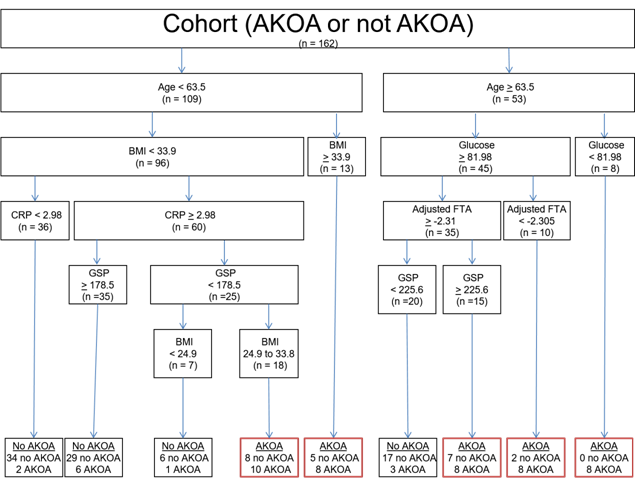
Results: Based on the CART analysis, the most important baseline variables for classifying individuals with incident accelerated KOA (in order of importance) were BMI, glucose concentrations, and age (Figure 1). Individuals < 63.5 years of age were likely not to develop accelerated KOA, except when they were overweight. Individuals ≥ 63.5 years of age were more likely to develop accelerated KOA unless their glucose levels were > 81.98 mg/dL, had varus malalignment, and had GSP concentrations < 225.6 nMol/mL. The relative error (unexplained variance) of the CART = 63%.
Conclusion: Age, BMI, and serum assays may enable the classification of individuals who will develop accelerated KOA in the subsequent 4 years. Future studies should explore other novel risk factors that may help classify individuals at risk for accelerated KOA and recognize the complex inter-play between risk factors. Figure 1. Classification and Regression Tree for Accelerated Knee Osteoarthritis (AKOA) versus those without AKOA
To cite this abstract in AMA style:
Driban J, McAlindon TE, Amin M, Price LL, Eaton CB, Davis J, Lu B, Lo GH, Duryea J, Barbe M. Risk Factors Can Classify Individuals Who Develop Accelerated Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/risk-factors-can-classify-individuals-who-develop-accelerated-knee-osteoarthritis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/risk-factors-can-classify-individuals-who-develop-accelerated-knee-osteoarthritis/