Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: A symptom checklist and screening indices for anxiety (ANX), depression (DEP), and/or fibromyalgia (FM) on patient questionnaires such as a multidimensional health assessment questionnaire (MDHAQ) facilitate recording symptoms as formal medical history data, not available prior to information technology. MDHAQ data may be informative to address two problems in RA: a. primary RA symptoms of joint pain and functional disability may be seen in patients with comorbid joint damage and/or patient distress, which may elevate RA core data set measures and indices in the absence of inflammatory activity; b. rheumatoid factor (RF) or anti-cyclic citrullinated proteins (ACPA) are found in only 67-69% of RA patients (Meta-analysis: Nishimura et al Ann Int Med. 2007;146(11):797-808). Formal recording of specific symptoms may be analogous to laboratory testing to inform management decisions. The prevalence of non-inflammatory symptoms in RA patients with positive versus negative screens on MDHAQ ANX, DEP, and FM indices was analyzed.
Methods: All patients seen in the study setting complete an MDHAQ, which includes a 60-symptom checklist to record a review of systems and screen for adverse events of high-risk medications. The prevalence of each symptom was computed in all patients and compared in those who screened positive versus negative for any of the 3 MDHAQ indices, MAS2 (MDHAQ anxiety screen), MDS2 (MDHAQ depression screen) and/or FAST4 (fibromyalgia assessment screening tool). The 15 most common non-inflammatory-based symptoms reported by all patients were identified, after excluding symptoms likely to result from inflammation, e.g., joint swelling, muscle pain, muscle weakness, dry eyes, dry mouth, although recognizing that the included and excluded symptoms might have an inflammatory or noninflammatory origin in certain individual patients. The prevalence of each symptom was then compared in patients who screened positive for MAS2 for ANX , MDS2 for DEP, and/or FAST4 for FM versus negative for all 3 indices.
Results: Among all 173 RA patients, 40-50% reported neck pain, headaches, unusual fatigue, anxiety (by definition), dyspnea, depression (by definition), and problems with memory, 20-40% reported dizziness, problems with thinking, heartburn, cough, palpitations, and 15-19% problems with social activities (Table). Each of these symptoms was reported by more than 50% of patients who screened positive for ANX , DEP, or FM, and by fewer than 50% in those who screened negative (Table). More than 70% of patients who screened positive for ANX, DEP, and/or FM reported problems with thinking, memory, sleeping, and unusual fatigue, in addition to anxiety and depression (by definition), higher than the prevalence of rheumatoid factor or ACPA in RA.
Conclusion: Symptoms on a computer checklist can function as clues to the likelihood of ANX , DEP, or FM in patients with RA who may have elevated DAS28, CDAI, or RAPID3, but little or no inflammation, analogous to laboratory tests. The prevalence of symptoms in >70% of RA patients with ANX, DEP, and/or FM is higher than the prevalence of RF or ACPA in RA in a meta-analysis. This information can inform more rational patient management toward improved care and outcomes.
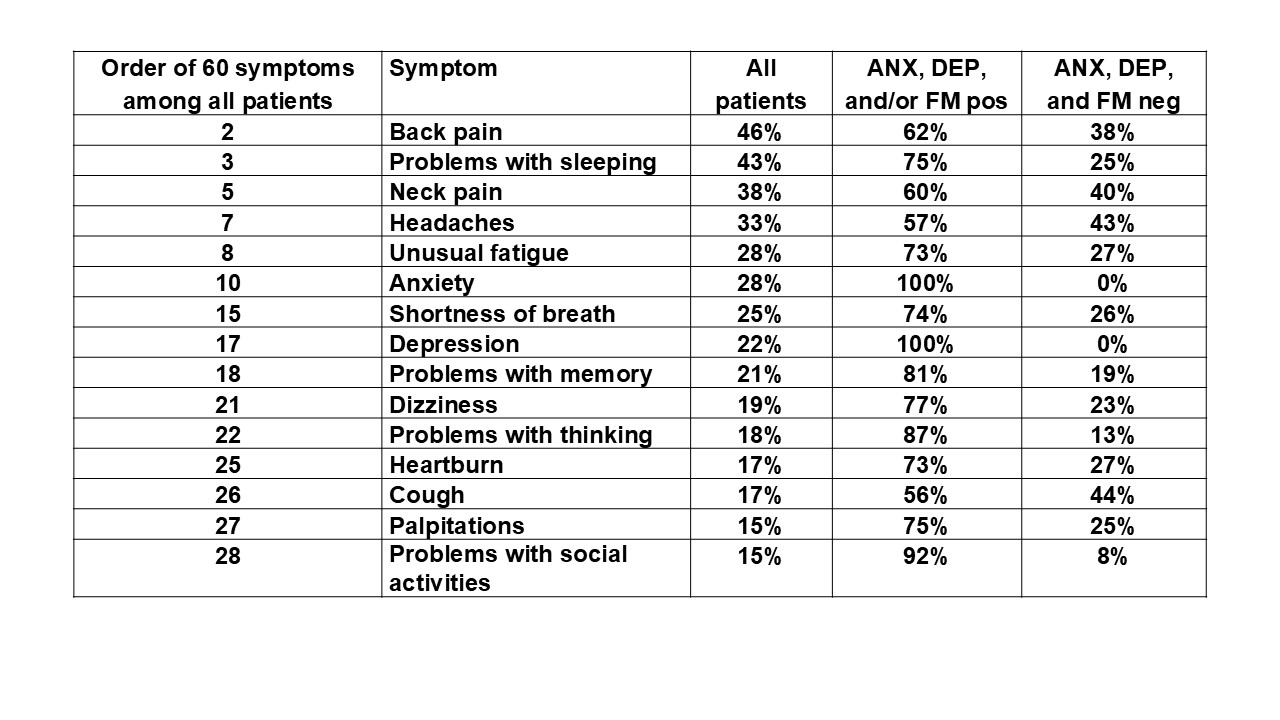 Prevalence of self-report of symptoms in 173 patients with rheumatoid arthritis on a multidimensional health assessment questionnaire (MDHAQ), including the order in all patients (symptoms reflecting inflammatory activity are such as joint pain as #1 are excluded) according to positive screening on 1 of 3 MDHAQ indices for anxiety (ANX), depression (DEP) and or fibromyalgia (FM)
Prevalence of self-report of symptoms in 173 patients with rheumatoid arthritis on a multidimensional health assessment questionnaire (MDHAQ), including the order in all patients (symptoms reflecting inflammatory activity are such as joint pain as #1 are excluded) according to positive screening on 1 of 3 MDHAQ indices for anxiety (ANX), depression (DEP) and or fibromyalgia (FM)
To cite this abstract in AMA style:
Pincus T, Schmukler J, Li T. Rheumatoid arthritis (RA) patients who screen positive for anxiety, depression, and/or fibromyalgia are more likely to report problems with sleeping, memory, and/or social activities than to have an abnormal rheumatoid factor or ACPA [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/rheumatoid-arthritis-ra-patients-who-screen-positive-for-anxiety-depression-and-or-fibromyalgia-are-more-likely-to-report-problems-with-sleeping-memory-and-or-social-activities-than-to-have/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheumatoid-arthritis-ra-patients-who-screen-positive-for-anxiety-depression-and-or-fibromyalgia-are-more-likely-to-report-problems-with-sleeping-memory-and-or-social-activities-than-to-have/