Session Information
Date: Friday, November 6, 2020
Title: Patient Outcomes, Preferences, & Attitudes Poster I: RA, Spondyloarthritis, & OA
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: The goal of this study was to examine whether cluster analysis could be used to identify homogeneous subgroups of engagement in RA patients enrolled in a digital health coaching program. The novelty of this approach was our attempt to identify actual user engagement behaviors, as opposed to employing engagement benchmarks derived from a trial protocol. These findings can help clinical staff stratify the RA population for digital health interventions between clinic visits for disease monitoring, self-management, and other efforts.
Methods: A longitudinal, retrospective analysis was conducted in a sample of RA members enrolled in Pack Health digital health coaching program (n = 66). Members reported the primary measures of RA disease severity (RAPID3) and physical and mental health quality of life (PROMIS) upon enrollment. Digital engagement data was measured using the frequency of outbound calls to a health coach, inbound calls from a health coach, the average call length, email open rate, frequency of outgoing patient text messages to a health coach, and incoming member text messages over the initial 12 weeks of the program. An agglomerative hierarchical cluster analysis was performed using Ward’s method to link and identify subgroups of members with similar profiles. Dismarilarity between RA members was calculated by the Minkowski distance in nine-dimensional space.
Results: Three clusters were identified with a Minkowski dissimilarity measure greater than 100. Cluster 1 (poor health, highly engaged) consisted of 28 patients with below-average PROMIS mental health (45.15), poor PROMIS physical health (38.70), and moderate to severe RA (RAPID3 4.90). This highly engaged cluster averaged 11.29 connected outbound calls or a 94% call success rate along with the highest volume of total text messages (56.75). Cluster 2 (better health, moderately engaged) consisted of 23 patients with below-average PROMIS mental health (46.50), above-average PROMIS physical health (52.49), and low RA severity (RAPID3 2.61). Cluster 2 averaged 8.48 total calls out of a possible 12 along with 16.3 total text messages. Cluster 3 (poor health, minimally engaged) consisted of 15 members with poor PROMIS mental health (32.05), poor PROMIS physical health (36.35), and high severity RA (RAPID3 4.90). This minimally engaged cluster averaged 3.07 successful calls and 15.2 total text messages. Complete health and engagement cluster data are shown in Table 1.
Conclusion: Results indicated that distinct patterns of engagement exist among RA patients in a digital health coaching program. The demographics and patient attributes identified in each subgroup may be helpful in (a) predicting RA patients’ participation and engagement in digital health interventions between clinic visits, and (b) enhancing patient engagement in digital health coaching programs for RA by tailoring treatment to the patient’s particular disease severity and engagement phenotype.
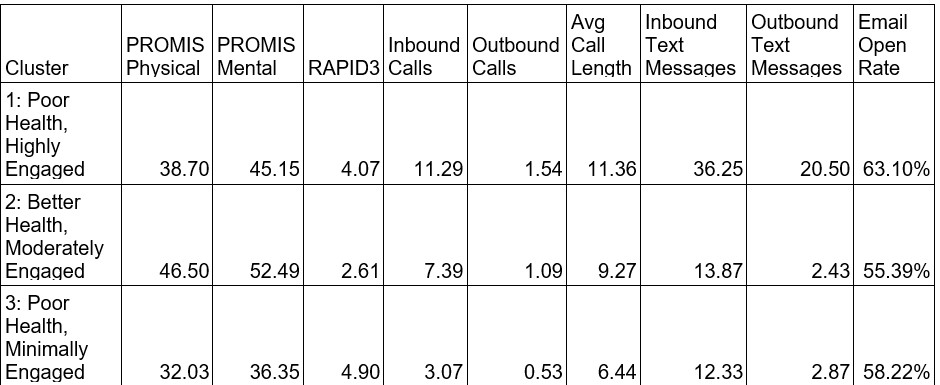 Table1: Cluster Descriptive Statistics
Table1: Cluster Descriptive Statistics
 Figure 1: Dendrogram for Hierarchical Cluster Analysis
Figure 1: Dendrogram for Hierarchical Cluster Analysis
To cite this abstract in AMA style:
Patterson J, Magid K, Patel D, Allison M. Rheumatoid Arthritis Patient Phenotypes from a Digital Health Coaching Engagement Program [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/rheumatoid-arthritis-patient-phenotypes-from-a-digital-health-coaching-engagement-program/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheumatoid-arthritis-patient-phenotypes-from-a-digital-health-coaching-engagement-program/