Session Information
Date: Sunday, November 13, 2022
Title: RA – Treatment Poster II
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Treatment efficacy for rheumatoid arthritis is often measured through disease assessments containing subjective input from the provider, the patient, or both. Here we compare scores from same-day CDAI and RAPID3 during treatment and at treatment discontinuation, to evaluate whether these disease assessments are aligned and are indicative of disease management.
Methods: Data are specific to patients in care by the American Rheumatology Network, and reside in PIONEER Rheumatology, an enhanced database combining fielded EMR data with extracted information from open text (office visits, infusions logs, and provider-patient communications). Study population: 61,312 patients with RA receiving conventional synthetic, targeted synthetic (ts), and/or biologic (b) DMARDs between 2014 to 2021 and with same day CDAI and RAPID3 scores. Total observations: 167,990 disease assessment scores, 83,995 patient-dates. Analyses conducted using R v.3.6: Spearman’s rho (score classifications), Pearson correlation (numeric scores), and Cohen’s weighted Kappa (score classification). Discontinuation analyses were limited to ts/bDMARD episodes and scores considered were closest to but between -90 to +14 days of discontinuation. Rapid3 and CDAI were split into low/remission, moderate, and severe disease activity.
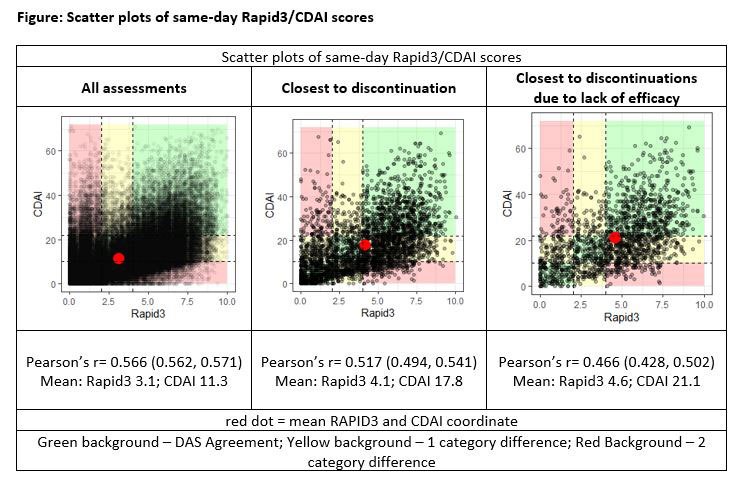
Results: A moderate agreement between same day CDAI and RAPID3 scores was suggested by Cohen’s Weighted Kappa (0.42) and Spearman’s rho (0.49). By disease severity classifications, a greater proportion of RAPID3 results indicated severe disease (35.8%; 30,057/83,995) v. CDAI (13.8%; 11,618/83,995; p< 0.001). Of the severe results by RAPID3, 25.6% (7683/30,057) were recorded as near-remission/low activity by CDAI. Conversely, 15.6% (1,818/11,618) of CDAI results indicating severe disease were classified as near-remission/low by RAPID3. In subset analyses examining scores at ts/bDMARD discontinuation (n=3600 drug episodes), 53.9% (1,939/3,600) had an accompanying RAPID3 result indicating severe disease compared to 31.6% by CDAI (1,136/3,600; p< 0.001). Of the 3,600 episodes, 47% (1,692) discontinued due to lack or loss of efficacy, as documented in visit notes; the remainder discontinued for non-clinical reasons and/or conditions arising from treatment, disease, or existing patient burden. For ts/bDMARD episodes discontinued for efficacy reasons, 19.6% (332/1,692) had an accompanying RAPID3 result indicating near-remission/low activity and 21.1% (356/1,692) indicated near-remission/low activity by CDAI (p=0.273). Scatter plots of individual scores are provided in the FIGURE.
Conclusion: A moderate correlation was observed between RAPID3, a patient-based disease assessment, and CDAI, a predominantly physician-based disease assessment. However, considerable discord was observed for ~10% of assessments, calling into question which assessment is a better indicator of disease management. Moreover, 20% of ts/bDMARD episodes that discontinued due to lack or loss of efficacy had near-remission/low disease activity by either RAPID3 or CDAI. These data suggest that some patient-important outcomes are not reflected in these assessments.
To cite this abstract in AMA style:
Soloman N, Huston K, singh J, Helfgott S, Frick A, Milligan S, Edgerton C. Review of 167,990 Same Day RAPID3, CDAI Scores for 61,312 Patients Receiving DMARD Treatment for Rheumatoid Arthritis; Evaluations of Disease Assessments and Treatment Discontinuation [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/review-of-167990-same-day-rapid3-cdai-scores-for-61312-patients-receiving-dmard-treatment-for-rheumatoid-arthritis-evaluations-of-disease-assessments-and-treatment-discontinuation/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/review-of-167990-same-day-rapid3-cdai-scores-for-61312-patients-receiving-dmard-treatment-for-rheumatoid-arthritis-evaluations-of-disease-assessments-and-treatment-discontinuation/