Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Systemic lupus erythematosus (SLE) is a systemic autoimmune disease with multi organ involvement. One of the most common manifestations is pulmonary disease with a reported prevalence between 5 – 90%. Given this wide range of prevalence, there is a need to more closely define types of pulmonary disease in SLE and associated risk factors. We sought to characterize the presentation of pulmonary manifestations in an established SLE cohort using electronic health record data.
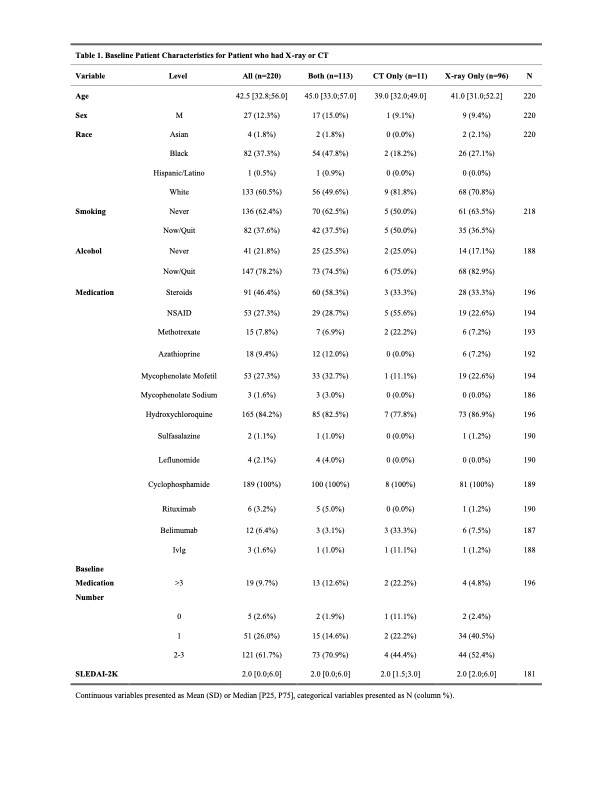
Methods: A retrospective chart review was performed using The Cleveland Clinic Health System electronic medical record data and the Cleveland Clinic Lupus Cohort (CCLC) data. All patients were >18 years of age and had confirmed SLE by a Cleveland clinic foundation rheumatologist using the 2012 SLICC or 2019 ACR/EULAR classification criteria. The cohort included 313 patients, 220 of whom had imaging studies completed. Generalized estimating equations (GEE) were utilized to analyze the data, accounting for its repeated measured nature.
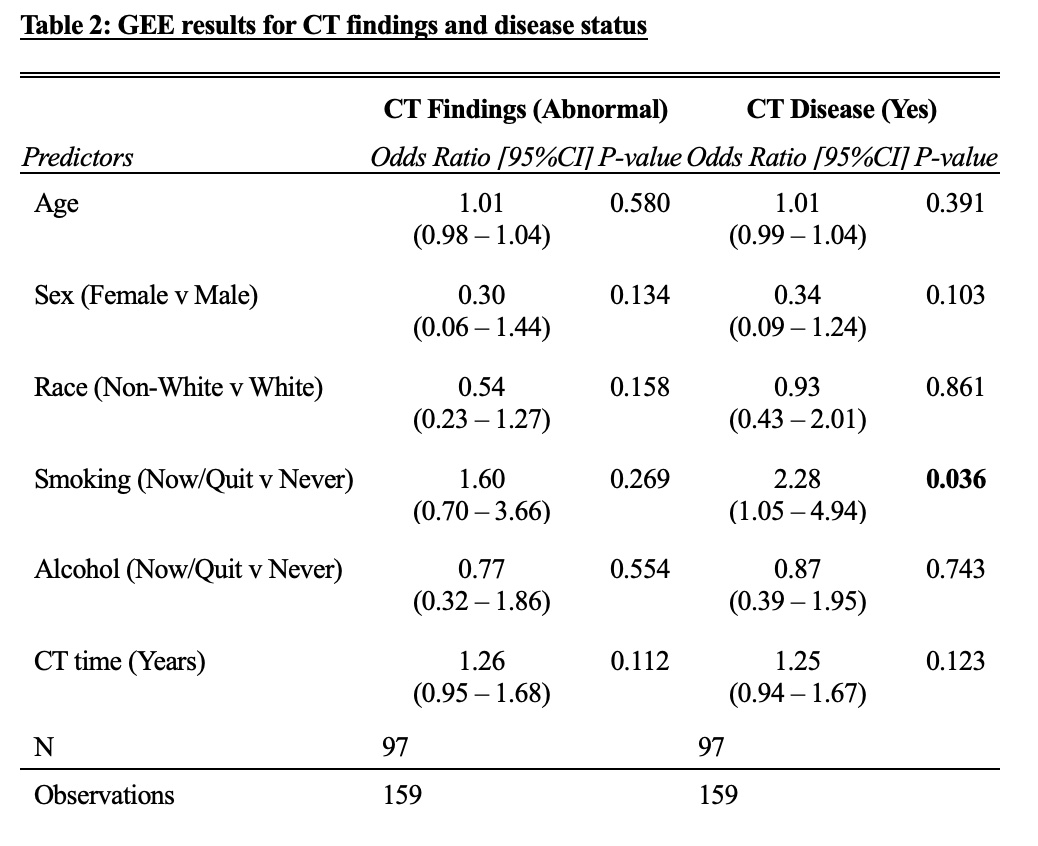
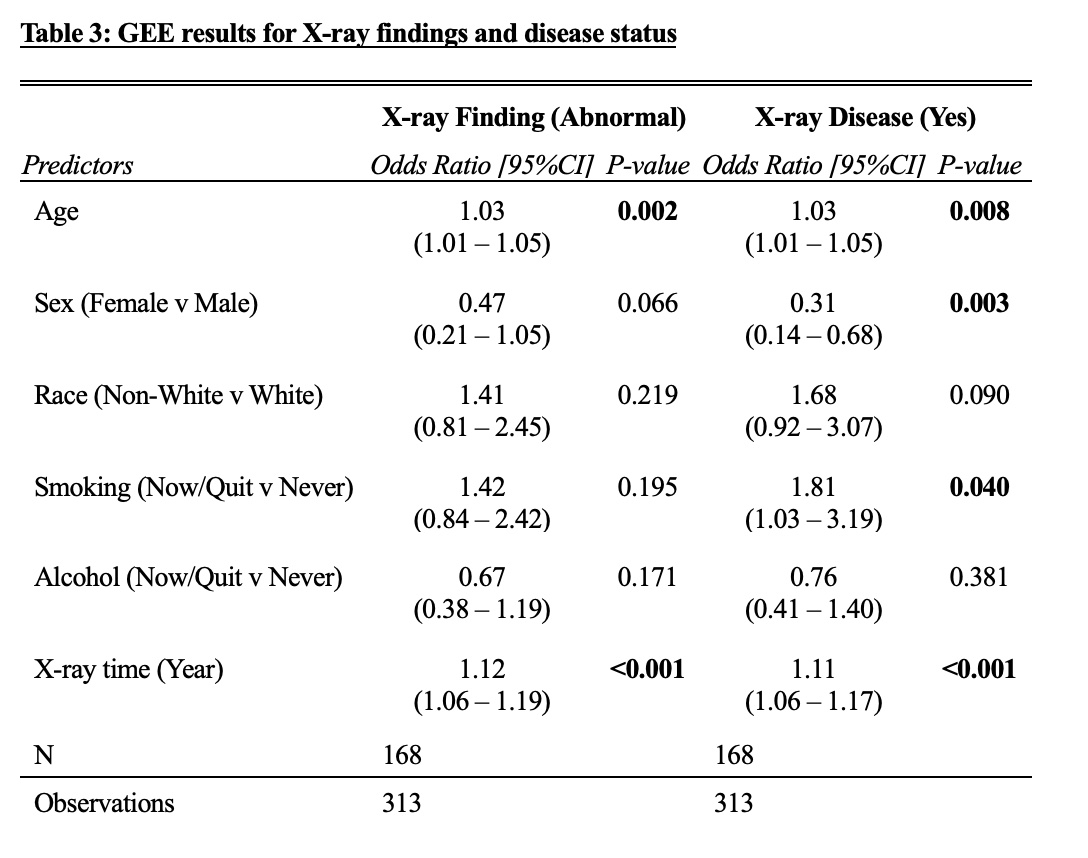
Results: The average age in our cohort was 42.5 years, 86.7% identified as female, 60.5% identified as white, 37.3% as Black, and 1.82% as Asian (Table 1). The most common findings on CT and x-ray were increased lung density (24%, 12%) and atelectasis (18%, 10%). The most common disease found on CT was pleural effusion (24%) or mediastinal/axillary lymphadenopathy (16%). Our GEE analysis showed no association between demographics and CT findings; however, patients who had smoked (current or former), had higher odds (OR 2.28, 95% CI: 1.05 – 4.94, p = 0.04) of radiologist reported disease on their imaging compared with patients who never smoked, even after adjusting for other covariates (Table 2). Additionally, the GEE results for disease on x-ray, as reported by the radiologist, showed that age, gender, smoking status, and x-ray time were significantly different in those who had a disease reported on their radiological report compared with those who did not (Table 3).
Conclusion: With the limited literature commenting on pulmonary involvement in SLE, our results show that certain factors, namely smoking, older age, and male sex should prompt clinicians to have a higher suspicion for lung disease in SLE patients. While our study is limited by the retrospective nature, lack of consistent SLEDAI-2K scores, and medication information within a date considered acceptable for inclusion in our analysis, our results highlight important characteristics for predicting pulmonary involvement in SLE. It is also important to note that the pathologies described herein cannot be directly attributed to SLE and could have secondary causes such as infection or other organ system failure. Further characterization in larger cohorts should be conducted to explore these possible associations. Until then, awareness of these potential risks is important for clinicians caring for SLE patients to optimize their care and follow up.
To cite this abstract in AMA style:
Johnson J, Zhang C, Littlejohn E. Retrospective Cohort Study Identifying Pulmonary Complications in a Cohort of Patients with Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/retrospective-cohort-study-identifying-pulmonary-complications-in-a-cohort-of-patients-with-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/retrospective-cohort-study-identifying-pulmonary-complications-in-a-cohort-of-patients-with-systemic-lupus-erythematosus/