Session Information
Date: Monday, November 14, 2016
Title: ACR/ARHP Combined Abstract Session: Epidemiology and Pubic Health
Session Type: ACR Concurrent Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Limb length inequality (LLI) is a condition in which one limb is longer than the other. Previous reports of a link between LLI and knee radiographic osteoarthritis (rOA) are limited by short follow-up durations. This longitudinal analysis examined the hazard of incident and progressive rOA and symptoms of the knee and hip by LLI in a large community-based cohort over a median 10-year follow-up period.
Methods: Participants were African American and Caucasian men and women 45+ years old enrolled from 1991-1997 (original cohort) or 2003-2004 (enrichment cohort), and follow up data were collected during 1999-2004, 2006-2010, or 2012-2015 (median follow-up time = 10 years, range= 4-22 years). Lower extremity lengths were measured with a tape measure from anterior superior iliac spine to distal medial malleolus with the participant supine; LLI was defined as ≥ 2 cm difference between limbs. Radiographs (anteroposterior [AP] standing knee and AP supine pelvic) were read for Kellgren-Lawrence grade (KLG). Incident rOA was defined as KLG <2 at baseline that becomes KLG ≥2 at follow-up. Progressive OA was defined as ≥ 1 KLG increase with baseline KL=1. Incident symptoms were defined as new symptoms (pain, aching, or stiffness on most days) at follow-up among joints without symptoms at baseline. Progressive symptoms were defined as joints with mild or moderate baseline symptoms that increased ≥1 level of severity (to moderate or severe) at follow-up. Separate parametric Weibull time-to-event models estimated hazard ratios of the association of LLI and knee and hip outcomes, adjusting for cohort (original or enrichment), time of LLI assessment (1991-1997 or 1999-2004), age, sex, race, and body mass index (BMI). In models where symptoms were the outcome, rOA was included as a covariate. Interactions between LLI and covariates were examined (p<0.10 considered statistically significant).
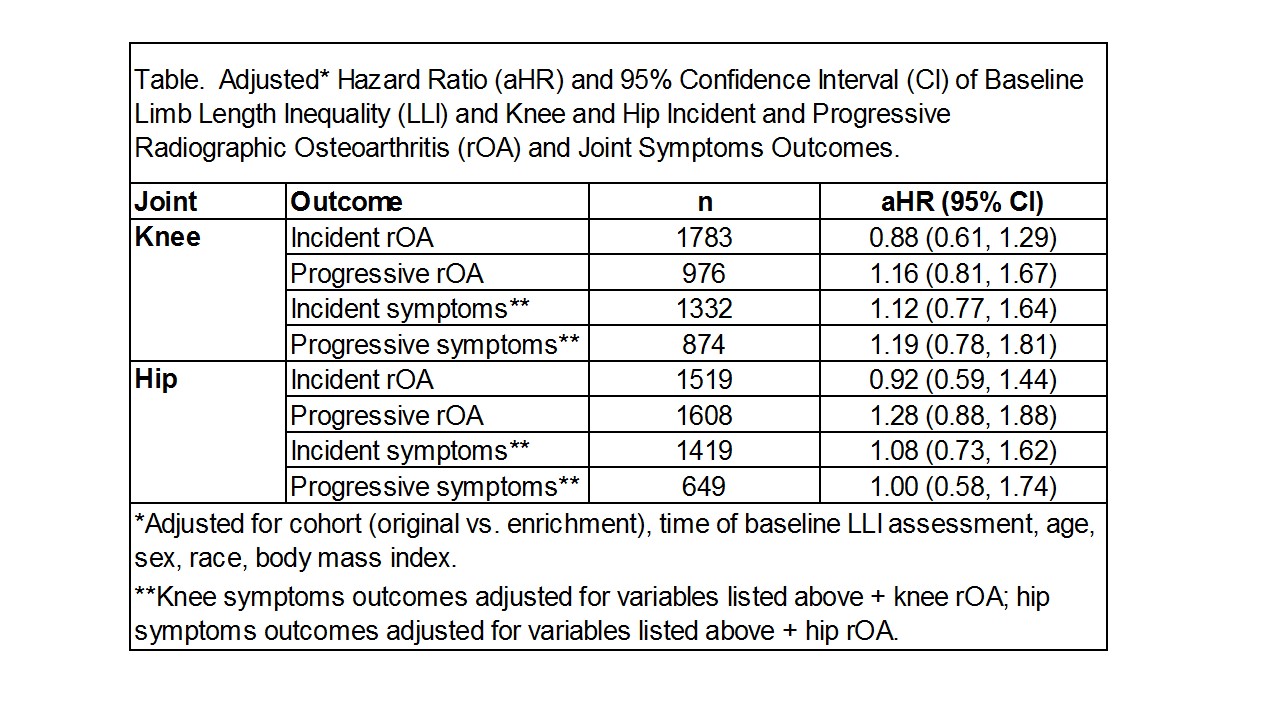
Results: At baseline, complete LLI with knee and hip radiograph data were available for 2872 and 2669 participants with at least one follow-up, respectively. Characteristics of the pooled sample were: mean ± standard deviation (SD) baseline age 61 ± 9.8 years; 2/3 women; 1/3 African American; mean ± SD baseline BMI 30 ± 6.4 kg/m2, and 7% with a LLI. The hazards of incident or progressive knee or hip rOA and symptoms by LLI were not statistically different (Table). There was a statistically significant interaction between LLI and BMI for progressive knee rOA; thus, results were stratified by BMI (<30 and ≥30 kg/m2). Among participants with BMI≥30, the adjusted hazard for progressive knee rOA was 76% higher among those with LLI vs. no LLI (adjusted hazard ratio 1.76, 95% confidence interval 1.12, 2.75).
Conclusion : Among obese participants, LLI was associated with progressive knee rOA. These results suggest that obese individuals with knee rOA and LLI may benefit from interventions to limit rOA progression.
To cite this abstract in AMA style:
Golightly YM, Alvarez C, Allen K, Renner JB, Jordan JM. Relationship of Limb Length Inequality and Incident and Progressive Knee and Hip Radiographic Osteoarthritis and Symptoms [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/relationship-of-limb-length-inequality-and-incident-and-progressive-knee-and-hip-radiographic-osteoarthritis-and-symptoms/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relationship-of-limb-length-inequality-and-incident-and-progressive-knee-and-hip-radiographic-osteoarthritis-and-symptoms/