Session Information
Date: Monday, November 13, 2023
Title: (1013–1032) Healthcare Disparities in Rheumatology Poster II: Socioeconomic Determinants
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Compared to non-Hispanic White children, Black children diagnosed with juvenile idiopathic arthritis (JIA) have more severe disease at diagnosis and worse outcomes, such as long-term disability. We aimed to determine if time to JIA diagnosis was longer in Black and Hispanic/Latinx populations and helped explain higher disease activity scores in minoritized populations.
Methods: We performed a retrospective cohort study using the CARRA registry, which contains sociodemographic, clinical, and patient/caregiver-reported data on children with pediatric-onset rheumatic diseases across the US and Canada. Eligible participants needed to have JIA, live in the US, and have complete data on self-reported race, ethnicity, and dates of symptom onset and diagnosis. We compared time to diagnosis among children in different racial and ethnic groups using Wilcoxon rank-sum testing, Kaplan-Meier curves, and multivariable Cox regression adjusted for age, sex, insurance type, self-reported household income and parental education, JIA type, calendar year of diagnosis, presence of uveitis, and local area-linked urban-rural status and socioeconomic disadvantage (Area Deprivation Index). To examine whether time to diagnosis mediated the relationship between race/ethnicity and disease activity at enrollment, we used a product of coefficients model, adjusting for the above covariates and time since JIA diagnosis, with bootstrapping to create bias-corrected 95% confidence intervals (CIs). Disease activity was assessed by Clinical Juvenile Arthritis Disease Activity Score 10 (cJADAS10). Missing data was imputed in 10 datasets using multiple imputation by chained equations.
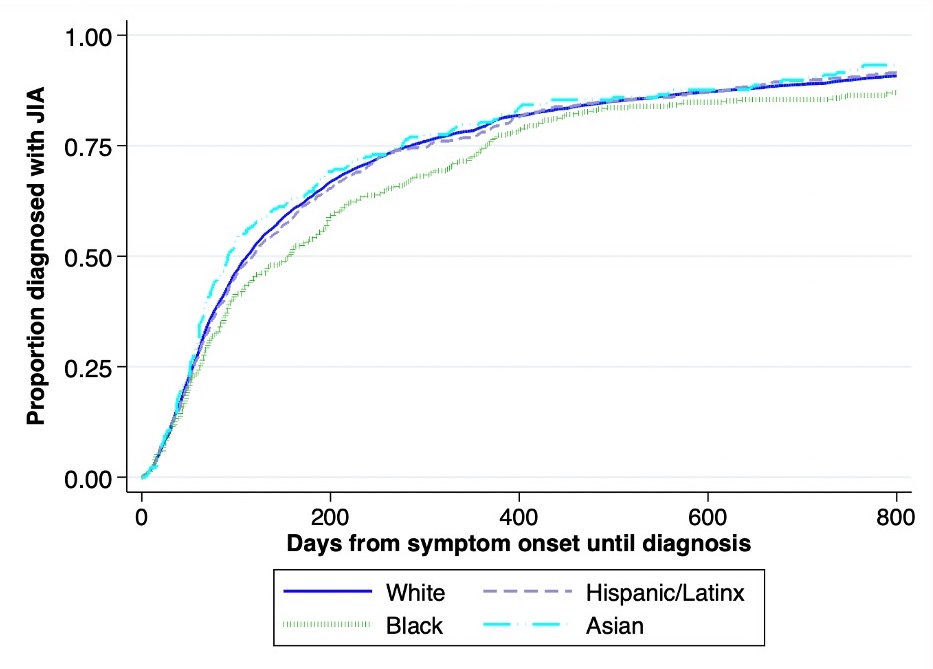
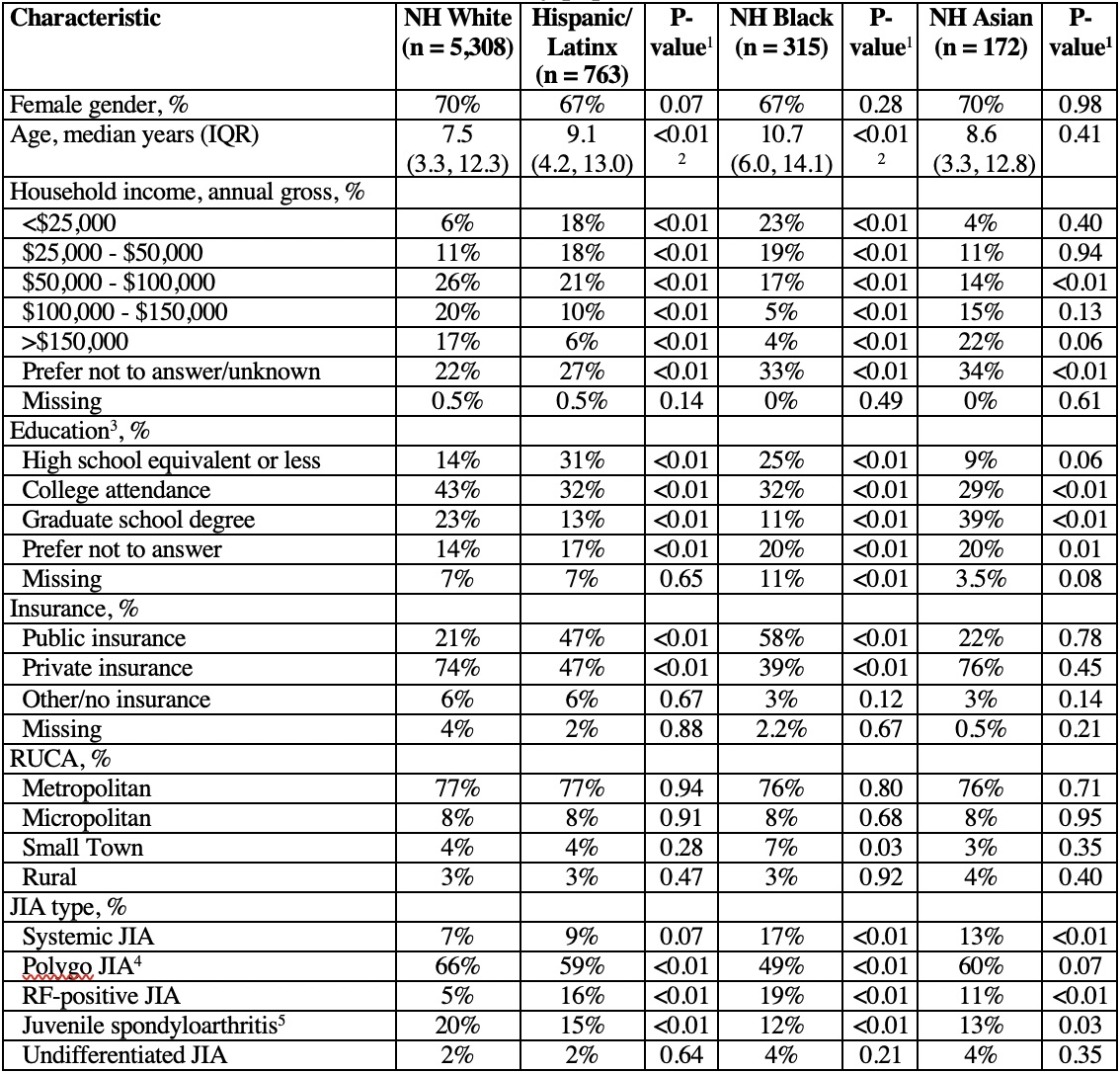
Results: Of 9,037 US Registry participants with JIA, 6,558 (73%) were included. Groups differed in baseline characteristics, including age, income, education, insurance status, and JIA type (Table 1). Compared to non-Hispanic White participants, non-Hispanic Black participants had higher median times to JIA diagnosis (156 days [interquartile range (IQR) 62, 365] vs. 112 days [IQR 54, 286], p=0.006) while times to diagnosis among other racial/ethnic groups were similar (Figure, Table 2). In adjusted models, non-Hispanic Black participants had a significantly longer time to diagnosis than non-Hispanic White participants (aHR 0.87, 95% CI 0.77, 0.98) (Table 2). Time to diagnosis partially mediated the association between Black race and cJADAS10 at enrollment (indirect coefficient = 0.08, bias-corrected 95% CI 0.03, 0.17), but this effect was considerably smaller than the direct relationship between Black race and cJADAS10 (direct coefficient = 1.67, 95% CI 1.50, 1.84).
Conclusion: In a large US cohort, Black children with JIA were more likely to experience delays in diagnosis independent of clinical, geographic, and socioeconomic factors. Higher disease activity scores in Black children at enrollment were modestly explained by longer times from symptom onset to diagnosis, but other factors appeared to contribute more substantially to these disparities. Future research should examine the role of systemic racism and other factors driving racial disparities in JIA diagnosis and disease activity as well as ways to address these factors.

To cite this abstract in AMA style:
McGuire S, Atanassova T, Madej J, Jimenez M, Horton D, the CARRA TMJ Arthritis Workgroup f. Relationship Between Race and Ethnicity, Time to Diagnosis, and Disease Activity for Children with Juvenile Idiopathic Arthritis in the CARRA Registry [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/relationship-between-race-and-ethnicity-time-to-diagnosis-and-disease-activity-for-children-with-juvenile-idiopathic-arthritis-in-the-carra-registry/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relationship-between-race-and-ethnicity-time-to-diagnosis-and-disease-activity-for-children-with-juvenile-idiopathic-arthritis-in-the-carra-registry/