Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Obesity [defined by body mass index (BMI) ≥30 kg/m2] is an established risk factor for incident radiographic knee OA (ROA). However, the relative contributions to ROA risk from increased joint load with higher body weight or systemic inflammation related to adipokines from excess fat mass (FM) are not well understood. We aimed to evaluate the extent to which ROA risk differs by FM for a given BMI or weight category in a longitudinal cohort to disentangle the effects of overall body mass from the potential effects of relative FM itself.
Methods: We included participants from the Multicenter Osteoarthritis Study (MOST), a NIH-funded longitudinal cohort of individuals with or at-risk for knee OA, who had DXA-measured body composition and were free of ROA at baseline [defined as Kellgren-Lawrence (KL) grade <2]. Incident ROA was identified by knee replacement or ROA (KL grade ≥ 2) occurring over 7 years in those free of baseline ROA. We stratified the sample by sex, and then created sex-specific BMI categories (i.e., < 25, 25-29.9, 30-34.9, ≥35 kg/m2). Within each BMI category, we computed %FM quartiles. We evaluated the relation of %FM quartiles (lowest quartile as referent) within each BMI category to risk of incident ROA using modified Poisson regression, adjusting models for age. We also evaluated for linear test for trend of increasing FM within BMI categories, and conducted sensitivity analyses examining incident ROA risk within categories of body weight (i.e., < 70, 70-79.9, 80-89.9, and ≥90 kg in females; < 90, 90-99.9, ≥100 kg in males).
Results: We included a total of 1611 people who had at least one knee free of ROA at baseline (2646 knees), mean age 61.7 years, 60% female, mean BMI 29.6 kg/m2 (Table 1). Incident ROA developed in 27.6% of participants over 7 years of follow-up. No differential risk of incident ROA was found by FM quartile within BMI categories (Figure 1). An exception was found among females with BMI 30-34.9 kg/m2, where those in the highest quartile of FM had 1.46 times the risk of incident ROA compared with the lowest quartile (adjusted RR 1.46, 95%CI 1.01-2.1). There were no significant linear trends in any of the BMI categories. Similar patterns were noted with weight categories (Figure 2).
Conclusion: Overall, higher fat mass within BMI or weight categories was not associated with increased risk for incident ROA. This suggests that total mass is likely more important for risk of ROA, primarily acting as a load contributor rather than metabolic influence from relative FM. Based upon these data, fat mass itself did not appear to increase risk of incident ROA substantially beyond risk conferred by BMI or body weight itself.
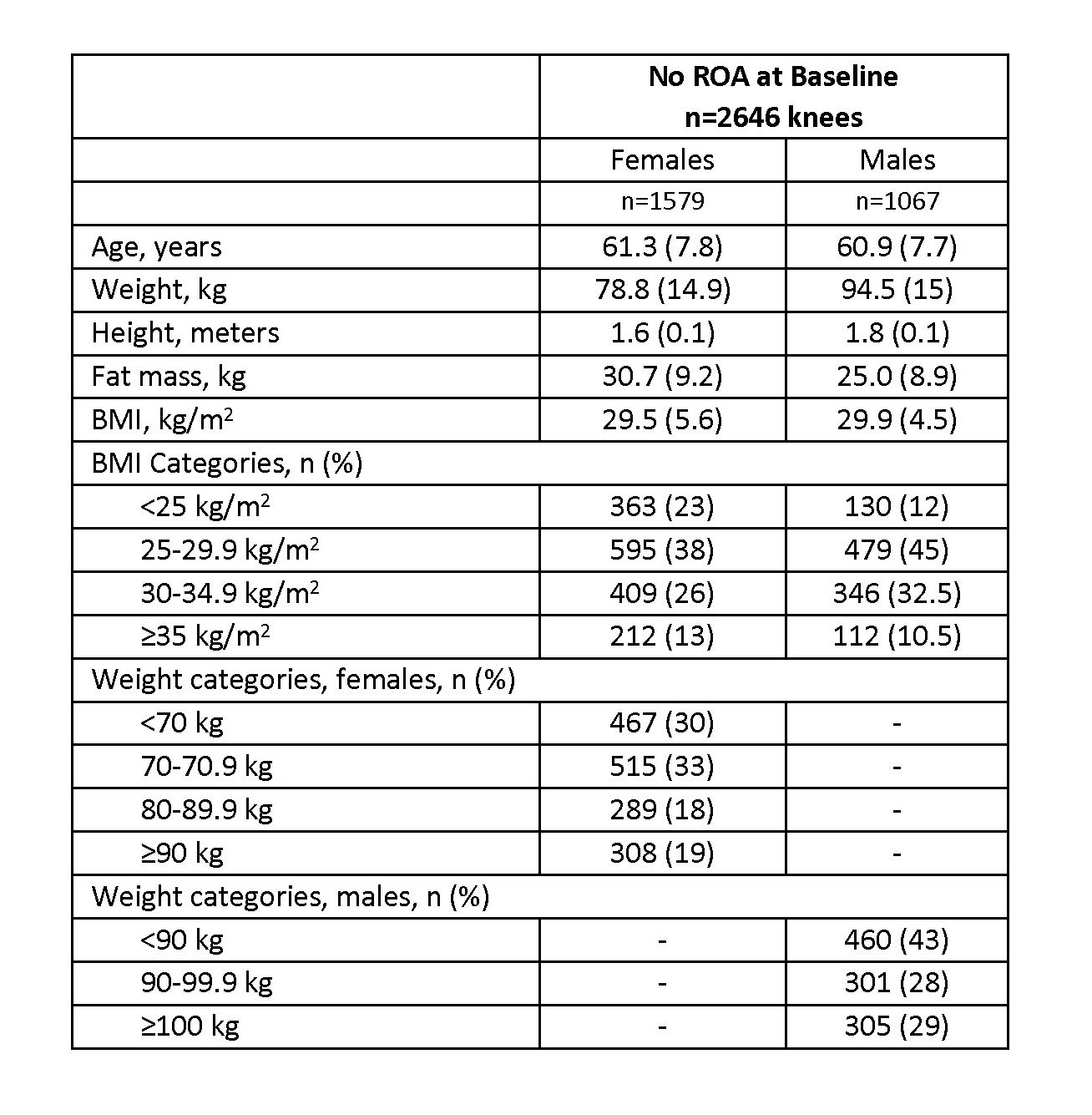
Values are reported as mean (standard deviation) unless otherwise indicated
Abbreviations: BMI = body mass index, ROA = radiographic knee osteoarthritis
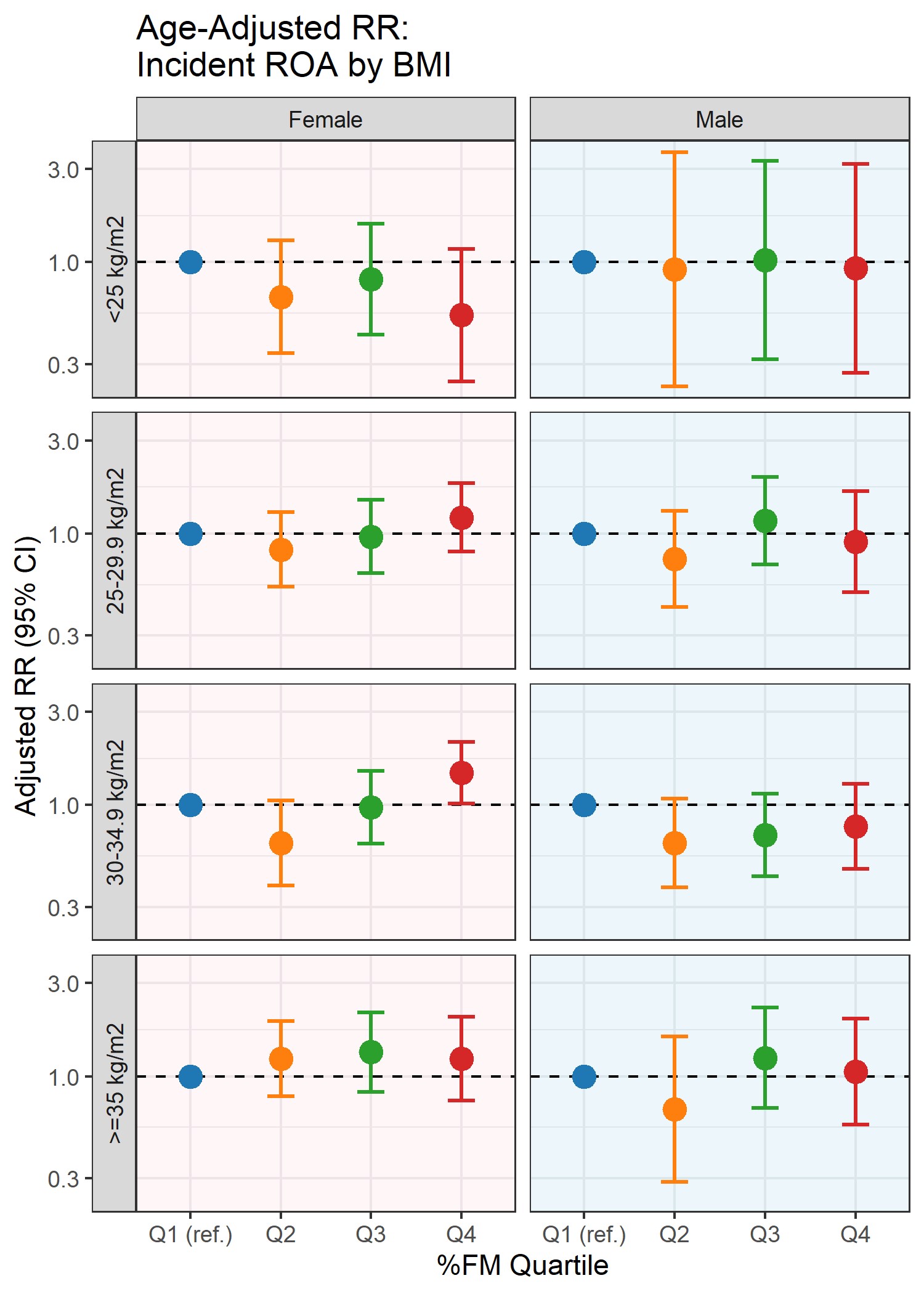
*Quartile 1 (lowest fat mass) was the reference for comparisons between quartiles 2,3, and 4 (highest fat mass)
Error bars show 95% confidence intervals (CI) for risk ratios.
BMI = body mass index, FM = fat mass, ROA = radiographic knee osteoarthritis, RR = risk ratio
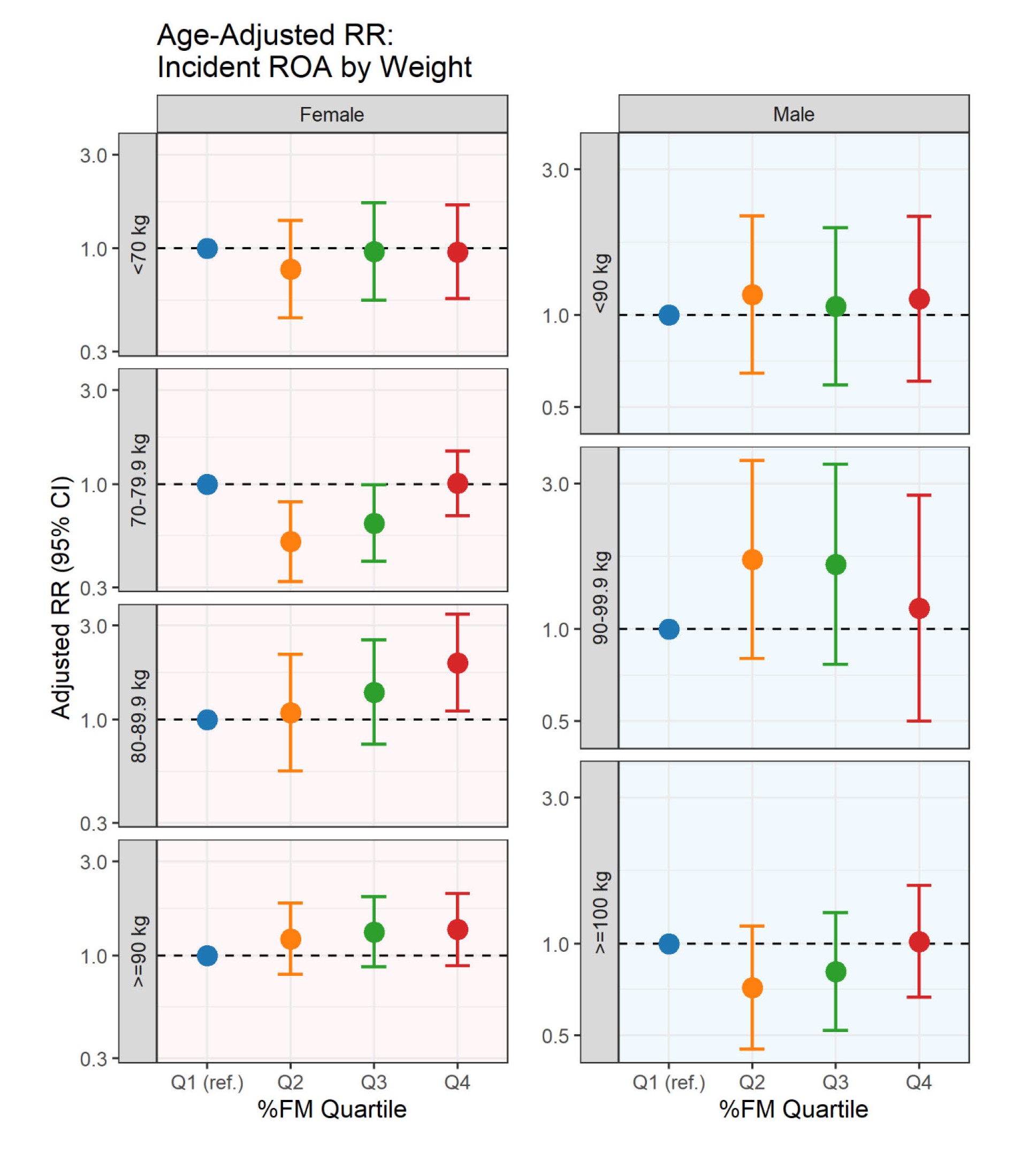
*Quartile 1 (lowest fat mass) was the reference for comparisons between quartiles 2,3, and 4 (highest fat mass)
Error bars show 95% confidence intervals (CI) for risk ratios.
FM = fat mass, ROA = radiographic knee osteoarthritis, RR = risk ratio
To cite this abstract in AMA style:
Godziuk K, Tilley S, LaValley m, Kiel D, Nevitt M, Lewis C, Torner J, Neogi T. Relationship Between Measures of Fat Mass and Knee Osteoarthritis Incidence: The Multicenter Osteoarthritis (MOST) Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/relationship-between-measures-of-fat-mass-and-knee-osteoarthritis-incidence-the-multicenter-osteoarthritis-most-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relationship-between-measures-of-fat-mass-and-knee-osteoarthritis-incidence-the-multicenter-osteoarthritis-most-study/