Session Information
Date: Monday, October 27, 2025
Session Type: Abstract Session
Session Time: 10:15AM-10:30AM
Background/Purpose: Mosaic loss of the Y chromosome (mLOY) is the most common acquired somatic mutation. Epidemiological studies have linked mLOY to malignancies, as well as cardiovascular and chronic kidney disease. Mechanistically, mLOY leads to the loss of epigenetic regulators on the Y chromosome, resulting in proinflammatory and profibrotic signaling. This evidence suggest a broader role for mLOY in age-related immune dysregulation and inflammation. In this context, giant cell arteritis (GCA) is a compelling candidate for further investigation, as it exclusively affects individuals over 50. This study is the first to assess the prevalence, clinical impact and pathophysiological consequences of mLOY in GCA.
Methods: Male patients with a diagnosis of GCA were enrolled. Demographic, clinical and imaging data were collected. Blood samples were obtained at the time of inclusion. Extraction and quantification of DNA was performed. Extent of mLOY was assessed using a digital droplet PCR with a SNP-based assay targeting a 6 bp difference between the AMELX and AMELY genes. The extent of mLoY was calculated as 1 − [AMELY]/[AMELX]. Cytokine concentration in the blood serum of GCA patient were assessed using the LEGENDplex™ Human Inflammation Panel 1.
Results: A total of 74 male patients with GCA (mean age 76.6 ± 10.7 years) were enrolled. At time of inclusion, 25.7% (19/74) exhibited active disease. During a mean follow-up of 599 ± 607 days, 24.3% (18/74) experienced at least one relapse, with a median time to relapse of 361 days (95% CI: 56.2–1470). The median mLOY burden was 17.8% (±23.7%). Receiver operating characteristic (ROC) analysis and Youden’s index identified an optimal mLOY threshold of 10.2% for relapse prediction (AUC: 0.706, p = 0.006) with 39.2% (29/74) exceeding this threshold. Within three years, 43.1% of patients with mLOY >10.2% relapsed compared to 8.7% with mLOY < 10.2% (p < 0.001, Kaplan–Meier log-rank test). Median relapse-free survival was 647 days (95% CI: 468–827) for mLOY >10.2%, versus 992 days (95% CI: 898–1,087) for mLOY < 10.2%. In multivariable Cox regression adjusted for age and clinical covariates, mLOY >10.2% emerged as the only independent predictor of relapse (HR: 17.4; 95% CI: 3.5–86.0; p = 0.003). Multiplex cytokine analysis revealed a significant association between mLOY burden an IL-6 levels (p = 0.045, r = 0.24) in the overall cohort. Among patients in remission (n = 45), those with mLOY >10.2% had significantly higher IL-6 levels than those with lower mLOY (p = 0.010). In patients in remission receiving tocilizumab (n = 32), mLOY burden was associated with both IL-6 (p = 0.002, r = 0.54) and IL-17A (p = 0.026, r = 0.40).
Conclusion: This is the first study to identify mLOY as a strong and independent predictor of relapse in male GCA patients, with a threshold of 10.2% mLOY burden associated with significantly reduced relapse-free survival. Elevated mLOY levels correlated with proinflammatory signaling, including increased IL-6 and IL-17A expression, particularly in patients receiving tocilizumab. Our findings suggest that mLOY may play an active role in the immunopathogenesis of GCA and serve as a prognostic biomarker to stratify patients at high risk of relapse.
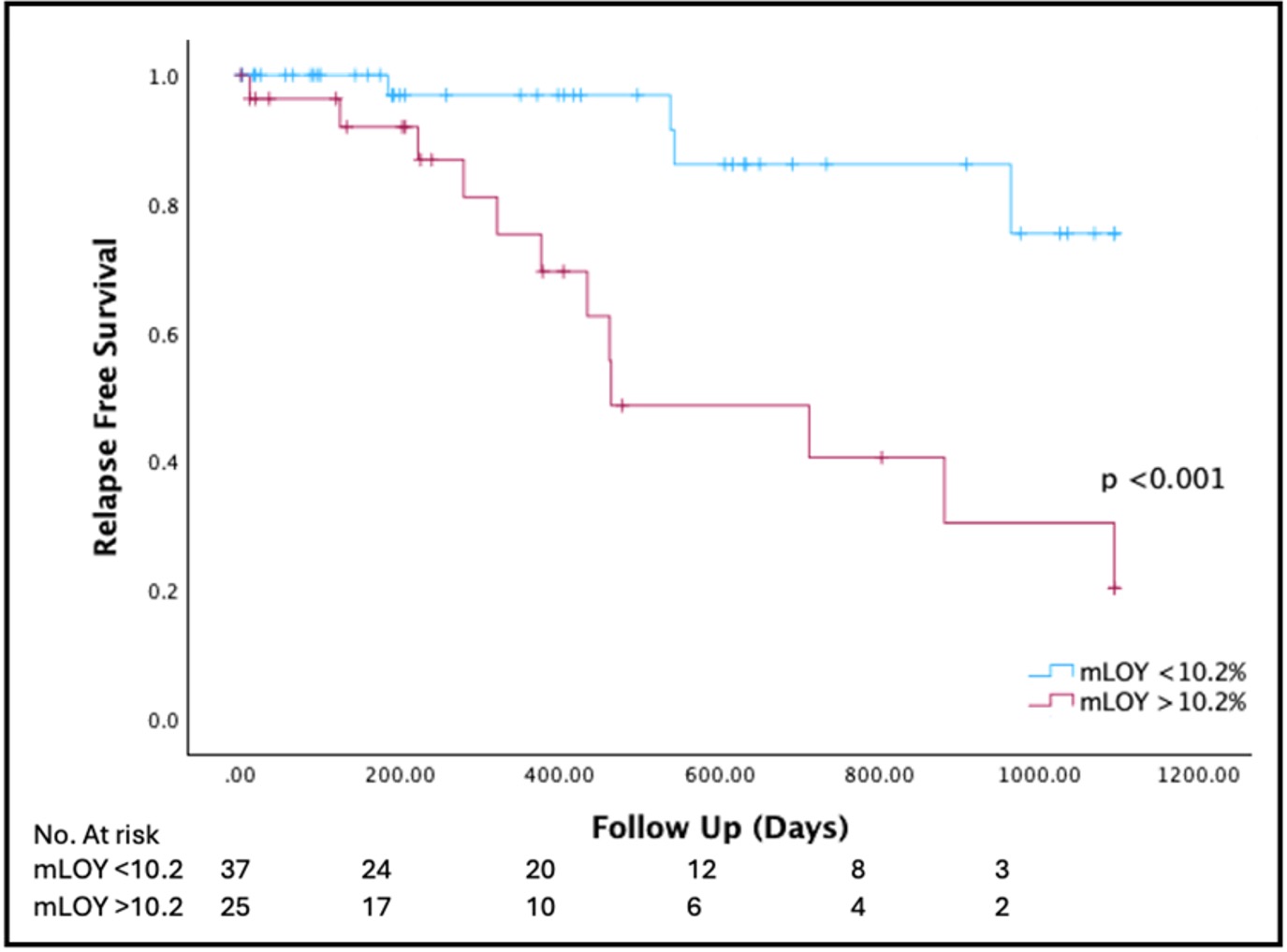 Figure 1: Survival Analysis for Predicting Relapse in Patients with Giant Cell Arteritis
Figure 1: Survival Analysis for Predicting Relapse in Patients with Giant Cell Arteritis
Figure 1 depicts the relationship between mLOY burden and relapse risk in GCA patients. Kaplan-Meier survival analysis demonstrates that patients with mLOY >10.2% had a significantly higher relapse risk (p < 0.001, univariate log-rank test) and a shorter median relapse-free survival (647 days [95% CI: 468–827]) compared to those with mLOY < 10.2% (992 days [95% CI: 898–1,087]; p < 0.001). Abbreviations: GCA = giant cell arteritis, mLOY = mosaic loss of Y chromosome, No. = number.
.jpg) Figure 2: Cox Regression Analysis for Risk Factors Associated with Relapse in Giant Cell Arteritis
Figure 2: Cox Regression Analysis for Risk Factors Associated with Relapse in Giant Cell Arteritis
This figure presents a Forest Plot summarizing the Cox regression analysis of relapse risk in patients with GCA, adjusting for factors potentially associated with relapse risk. The model included seven variables: age, mLOY burden > 10.2 %, CRP levels, visual impairment, constitutional symptoms (fever, night sweats, weight loss), large vessel vasculitis (LVV), and shoulder or pelvic pain. Abbreviations: Constit. Symptoms = constitutional sympttoms, HR = hazard ratio, mLOY = mosaic loss of the Y chromosome, CRP = C-reactive protein, VI = visual impairment, LVV = large vessel vasculitis, adj. p = adjusted p-value. *p < 0.05 indicates statistical significance.
.jpg) Figure 3: Inflammatory Cytokine Profile, Mosaic Loss of the Y Chromosome, and Clinical Parameters in Patients with Giant Cell Arteritis.
Figure 3: Inflammatory Cytokine Profile, Mosaic Loss of the Y Chromosome, and Clinical Parameters in Patients with Giant Cell Arteritis.
Figure 3 depicts inflammatory cytokines measured by LegendPlex shown as heatmap. Clinical parameters are depicted above columns. In the overall cohort, mLOY as a continuous variable was positively associated with IL6 (p = 0.045). * = p < 0.05 indicates statistical significance, Abbreviations: CRP= C-reactive protein, DA = disease activity, GCA = giant cell arteritis, IL = interleukin, Predn. = prednisolone, TCZ = tocilizumab, mg = milligram, mLoY = mosaic loss of the Y chromosome, Nfno, Y=yes, y = years.
To cite this abstract in AMA style:
Petzinna S, Kirch S, Adamson M, Xi D, Bauer C, Kreis L, Karakostas P, Behrendt R, Zimmer S, Jamin R, Schäfer V. Relapse and Immune Dysregulation in Giant Cell Arteritis Are Linked to Mosaic Loss of the Y Chromosome [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/relapse-and-immune-dysregulation-in-giant-cell-arteritis-are-linked-to-mosaic-loss-of-the-y-chromosome/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relapse-and-immune-dysregulation-in-giant-cell-arteritis-are-linked-to-mosaic-loss-of-the-y-chromosome/