Session Information
Date: Tuesday, October 28, 2025
Title: (2195–2226) Reproductive Issues in Rheumatic Disorders Posters
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Idiopathic Granulomatous Mastitis (IGM) is a rare benign inflammatory condition of the breast usually affecting women of childbearing age with a history of breastfeeding. It is characterized clinically by breast pain, erythema, mass(es), and recurrent or non-healing wounds, and is diagnosed histologically by the presence of non-necrotizing granulomatous lesions. It is theorized that when ductal epithelium is damaged, like in milk stasis, luminal secretions leak into surrounding lobular connective tissue and trigger the recruitment of macrophages and lymphocytes, causing local inflammation. It can be difficult to distinguish IGM from infectious mastitis or inflammatory breast cancer, often delaying diagnosis. The treatment of IGM largely consists of surgical intervention, local steroids, systemic steroids, and/or disease modifying anti-rheumatic drugs (DMARDs) without a universally accepted treatment algorithm.
Methods: Here, we present 8 patients evaluated in the NYU-Langone Long Island rheumatology academic office in 2025 diagnosed with IGM via histology and explore the patients’ demographics, management, and outcomes after referral to rheumatology via chart review. We obtained IRB approval, s25-00399. We reviewed imaging of the affected areas, histopathology, and microbiology data.
Results: 8 cases were included, all of which were biological females. 3 patients (37.5%) identified as Hispanic, 3 (37.5%) identified as Asian (including East and Southeast Asian), and 2 (25%) identified as European/Caucasian. 50% used oral contraception. Radiographic information from patients’ ultrasounds and/or mammograms was especially notable for 62.5% of cases containing tubular components, which is a more unique finding to IGM. 100% of patients underwent biopsy and histopathologic features included granulomatous inflammation (100%), fibrosis (25%), mastitis (25%), and necrosis (12.5%). All 8 patients in the series had healing of wounds, resolving of pain, and diminishing mass sizes. 7 patients (87.5%) were treated with prednisone with symptom improvement, with the addition of methotrexate in the 4 refractory cases (50%). 4 patients (50%) underwent multiple procedures including incision and drainage.
Conclusion: Greater understanding and recognition of IGM may expedite diagnosis and reduce morbidity. When histopathologic diagnosis of IGM is made, rheumatology referral should be made promptly. Our patients had a gap of approximately 10 weeks from diagnosis of IGM to first rheumatology visit, with no further surgical procedures after rheumatology medical management. Patients often underwent multiple procedures including incision and drainage prior to diagnosis, which in conjunction with the inflammatory state of the breast, led to high risk of poor wound healing. This suggests earlier rheumatological evaluation may lead to swift treatment with glucocorticoids and DMARDs, resolution of symptoms, and prevention of deformity from repetitive surgical procedures. Our case series adds data to the knowledge base about IGM and may contribute to the development of treatment guidelines for the future.
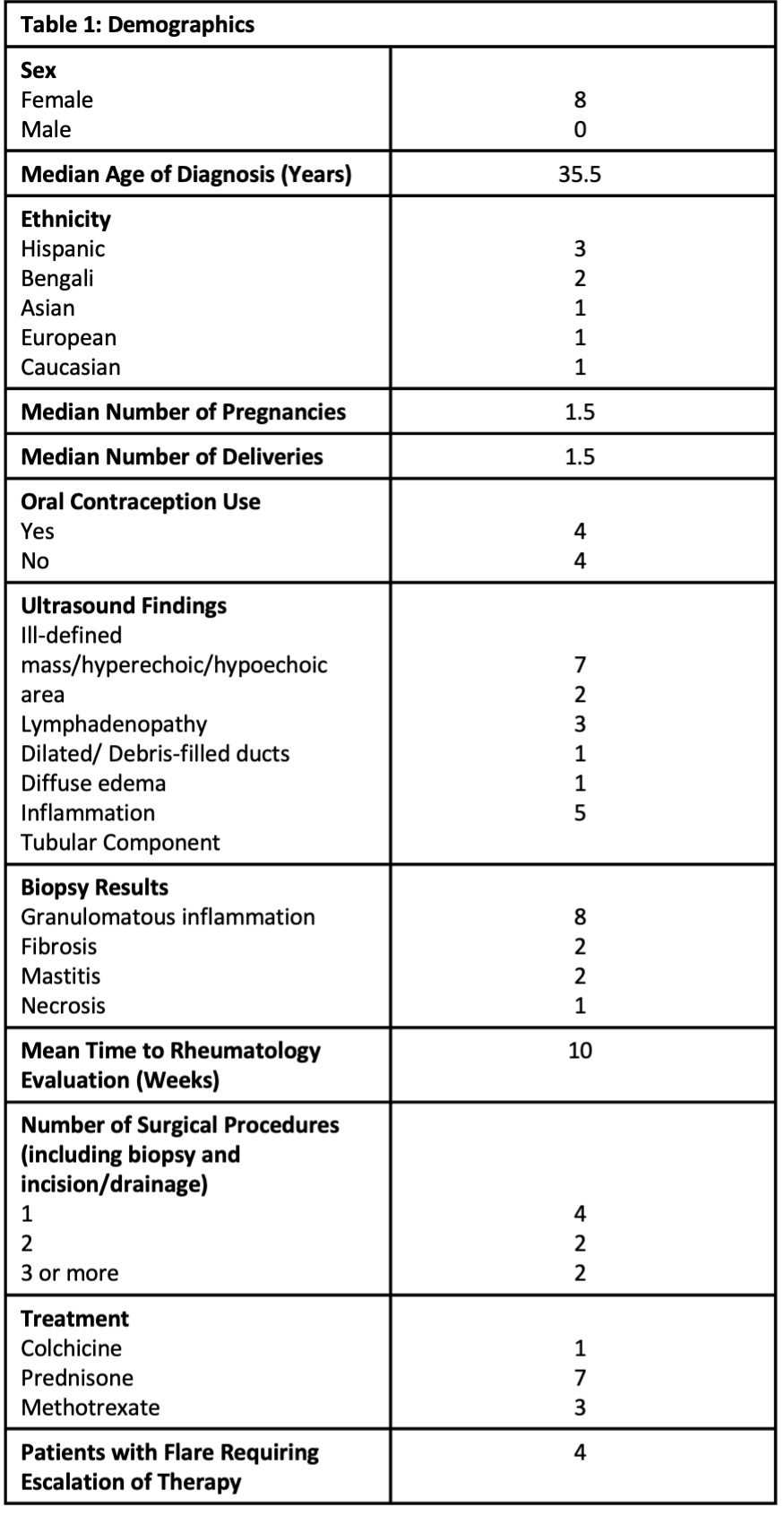 Table 1: Demographics
Table 1: Demographics
.jpg) Lobulocentric mastitis with acute and chronic inflammation evidenced by neutrophils and lymphocytes including few giant cells and focal ill-defined granuloma formation.
Lobulocentric mastitis with acute and chronic inflammation evidenced by neutrophils and lymphocytes including few giant cells and focal ill-defined granuloma formation.
To cite this abstract in AMA style:
Solomon J, Piccione J, Nusbaum J, Carsons S, Blumberg G. Recognition and Treatment of Idiopathic Granulomatous Mastitis: A Case Series [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/recognition-and-treatment-of-idiopathic-granulomatous-mastitis-a-case-series/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/recognition-and-treatment-of-idiopathic-granulomatous-mastitis-a-case-series/